ABSTRACT
Background: Surgical site infections (SSIs) are a major cause of postoperative morbidity, prolonged hospitalization, and increased healthcare expenditure. Appropriate use of surgical antibiotic prophylaxis (SAP) is a key strategy for SSI prevention. Despite clear recommendations in the Malaysian National Antibiotic Guidelines (NAG) 2024, adherence remains variable across institutions. Methods: A prospective observational study was conducted from April to June 2024. A total of 208 patients undergoing elective or emergency surgery were included. Data on demographics, surgical characteristics, wound classification, and antibiotic administration were collected. SAP appropriateness was assessed based on NAG 2024 and the institutional Antimicrobial Stewardship Policy. Descriptive statistics were generated, and associations between guideline compliance and clinical variables were analyzed using Chi-square and Fisher’s exact tests, with significance set at p < 0.05. Results: Only 23.1% of patients received guideline-compliant pre-operative prophylaxis, while 16.8% adhered to post-operative recommendations. A total of 205 and 179 instances of inappropriateness were identified in pre-operative and post-operative antibiotic use, respectively. Obstetrics and Gynaecology (O&G) contributed the highest proportion of inappropriateness in both phases (67.8% pre-operative; 59.2% post-operative). The most common reason for inappropriateness in pre-operative antibiotic prophylaxis was incorrect dosing (59.0%), followed by wrong antibiotic selection (12.2%) and incorrect timing (11.2%). Inappropriateness in the post-operative phase was predominantly due to antibiotics prescribed when not indicated (52.5%) and prolonged duration (40.8%). Significant associations with pre-operative non-compliance included discipline (p < 0.001), citizenship (p = 0.017), type of procedure (p < 0.001), and wound classification (p < 0.001). Notably, 82.2% of patients received antibiotics for more than 24 hours despite guideline recommendations. Conclusion: This study showed a low rate of SAP guideline compliance in this hospital. Pre-operative non-compliance was mainly driven by incorrect dosing and inappropriate antibiotic selection. In the post-operative phase, unnecessary continuation of antibiotics beyond 24 hours and prolonged duration were the most frequent prescribing errors.
INTRODUCTION
Surgical site infections (SSIs) are a major complication following surgical procedures and are closely associated with increased patient morbidity, prolonged hospitalisation, and a rise in healthcare costs. According to the Centers for Disease Control and Prevention (CDC), SSIs occur at or near the site of surgery within 30 days of the operation or within one year if an implant is involved [1]. These infections significantly affect recovery outcomes and can increase mortality risks [2]. An estimated 110,800 SSIs were associated with inpatient surgeries in 2015, according to the CDC healthcare-associated infection survey [1]. Local studies have reported prevalence rates of SSIs ranging from 13% to 17% [3,4,5]. In addition to clinical complications, SSIs impose a substantial healthcare burden through increased intensive care utilisation, higher readmission rates, prolonged antimicrobial exposure, and excess healthcare expenditure. Patients who develop SSIs have been reported to experience hospital stays extended by up to 7–11 days and significantly higher treatment costs compared to non-infected surgical patients, highlighting the importance of effective preventive strategies [6,7].
One of the most effective strategies for reducing the risk of SSIs is the appropriate use of antimicrobial prophylaxis. Despite established guidelines, the compliance rate for antibiotic surgical prophylaxis has been found to vary widely, ranging from 1.08% to 55.4%, with inappropriate duration of antimicrobial use being reported as the most common issue worldwide [8,9]. Prolonged or unnecessary surgical antibiotic prophylaxis does not confer additional protection against SSIs but instead increases the risk of antimicrobial resistance, Clostridioides difficile infection, drug-related adverse events, and selection pressure favouring multidrug-resistant organisms [10]. These practices contribute to the global issue of antimicrobial resistance (AMR).
Although the Malaysian National Antibiotic Guidelines (NAG) 2024 [11] provide clear directives, actual compliance remains inconsistent. Local studies have consistently shown misuse in terms of inappropriate antibiotic selection, incorrect administration timing and dosage, and prolonged usage beyond the recommended duration [2,3,4,5]. This is often due to outdated practices, inadequate knowledge dissemination, and the absence of localised clinical audits [8]. Without institution-specific monitoring, variations in prescribing practices often remain unrecognised, limiting the ability of antimicrobial stewardship programs to implement targeted interventions, optimise prescribing behaviour, and evaluate the effectiveness of guideline implementation at the local level [12].
Lahad Datu is a district located on the east coast of Sabah with a population of 299,550 [13]. Hospital Lahad Datu is the only hospital in the district serving the community. An outbreak of carbapenem-resistant Enterobacter (CRE) cases has occurred at Hospital Lahad Datu, in addition to the high usage of broad-spectrum antibiotics (e.g., meropenem). Furthermore, Hospital Lahad Datu has not previously conducted an audit of its surgical antibiotic prophylaxis practices. The absence of local audit data creates an important knowledge gap, as national or international compliance data may not accurately reflect prescribing behaviours, resource limitations, microbial epidemiology, or workflow practices unique to Hospital Lahad Datu. Without locally generated evidence, antimicrobial stewardship policies may lack contextual relevance, limiting their effectiveness in guiding clinical decision-making and resistance containment strategies. Therefore, conducting a structured audit is essential not only to measure compliance but also to generate actionable institutional data that can inform targeted stewardship interventions, optimise antibiotic utilisation, and support hospital-level policy refinement.
This study aimed to evaluate the appropriateness of surgical antibiotic prophylaxis (SAP) at Hospital Lahad Datu and to determine factors associated with guideline compliance. The audit assessed adherence to established recommendations regarding antibiotic selection, timing of administration, dosing, duration of therapy, and overall compliance with current guidelines. The findings are expected to provide evidence-based data to strengthen antimicrobial stewardship initiatives and support the future refinement of surgical antibiotic prophylaxis (SAP) policies at the institutional level.
METHOD
This prospective observational study was conducted at Hospital Lahad Datu, Sabah, over a three-month period between April 2024 and June 2024. A standardized surveillance form was used to facilitate data collection, and all patients were selected using a universal sampling method. Both adults and paediatric patients who were admitted for emergency and elective operations to the operating theatre, regardless of nationality, were eligible for inclusion in this study after obtaining informed consent. Patients who were transferred in from other facilities for postoperative care, or who had concurrent infections or contaminated/dirty wounds prior to the operation were excluded from this study. Since this study was an exploratory audit of surgical antibiotic prophylaxis practices at Hospital Lahad Datu, the sample size was not calculated.
Data Collection
All relevant data were retrieved from the patients’ medication charts and medical records. Details recorded included patients’ socio-demographic data, date of admission, surgical information (e.g., dates & type of surgery, wound class, duration of operation), prophylactic antibiotic administration details (e.g., antibiotic choice, route, dose, timing, indication for surgery, and guideline compliance), and relevant laboratory results. Data on post-operative antibiotic administration was also collected. Each patient was reviewed from the time of admission until their discharge from the hospital. The wound classification was based on the Centers for Disease Control (CDC) standards [14]. Guideline compliance and antibiotic appropriateness were evaluated for each patient with reference to the National Antibiotic Guidelines, Hospital Lahad Datu’s Antimicrobial Stewardship Policy, and other relevant references.
Outcome Measurement
Antibiotic appropriateness was evaluated for each patient according to compliance with the Malaysian National Antimicrobial Guidelines (NAG), Hospital Lahad Datu’s Antimicrobial Stewardship Policy, and other relevant references. This study assessed compliance with established antibiotic selection criteria, administration timing, dosing, duration of use, and overall adherence to current guidelines. Any case that met one or more of the reasons for inappropriateness was regarded as non-compliant with guidelines.
Ethical approval
The research has been approved by the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia, with the registration ID NMRR-23-03704-2BB.
Statistical Analysis
All data collected were analyzed using the Statistical Package for the Social Sciences (SPSS Inc., Chicago, USA) version 30. Data on demographic characteristics, surgical details, wound classification, antibiotic usage, and compliance with national and local guidelines were collected and analysed. Categorical variables were presented as counts and percentages, while numerical variables were presented as median with an interquartile range. Chi-square and Fisher’s exact tests were used to assess the associations between guideline compliance and independent variables, including discipline, citizenship, time of procedure, type of procedure, and wound classification. The level of statistical significance was set at p < 0.05 with a confidence interval (CI) of 95%.
RESULT
Sample Characteristics
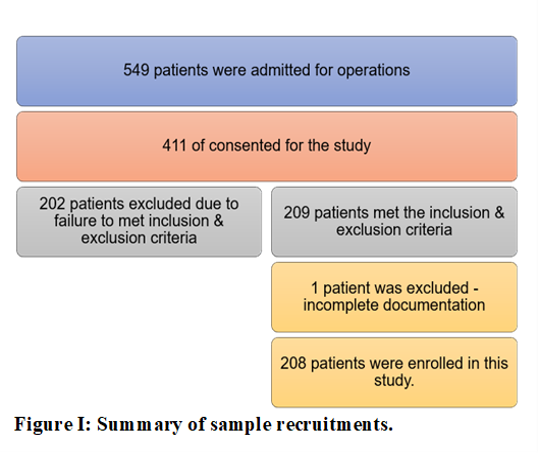
A total of 549 patients were admitted for operations throughout the study period, with 411 of them providing consent. Out of these, 209 patients met all the inclusion and exclusion criteria, and one patient was excluded due to incomplete documentation of antibiotic usage. Hence, 208 patients were enrolled in this study.
Demographic Characteristics
The demographic characteristics of the patients are shown in Table I. The median age of the patients in the study was 32 years, and the median body weight was 64.3 kg. Most patients in the study were female, comprising 70.7% (n=147), while male patients accounted for 29.3% (n=61).
The study population was predominantly local citizens at 68.3% (n=142), with the remaining 31.7% (n=66) being non-locals. Five disciplines participated in this chemoprophylaxis study. The highest number of patients came from the Obstetrics and Gynecology discipline, accounting for 58.7% (n=122), followed by Surgical 18.8% (n=39), Orthopedic (13.9%, (n=29), Otorhinolaryngology (4.8%, n=10), and the least from the Dental Department (3.8%, n=8). The study showed that a total of 97.6% (n=203) of cases were initial surgeries, and more than half of the procedures were emergency procedures, accounting for 56.3% (n=117). Additionally, 79.8% (n=166) of the cases were classified as clean contaminated surgeries, while 20.2% (n=42) were classified as clean surgeries. This study also indicates that 82.2% (n=171) of the patients received prophylactic antibiotics for more than 24 hours, while the remaining 17.8% (n=37) received prophylactic antibiotics for 24 hours or less.
Wound Classification Across Disciplines
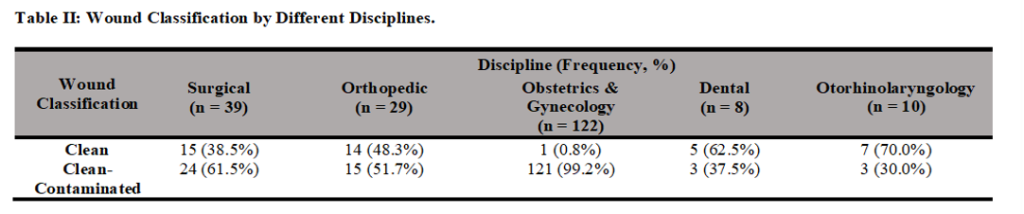
Table II shows the distribution of wound classification across the different surgical disciplines. Surgical (61.5%, n = 24), Orthopaedic (51.7%, n = 15), and Obstetrics & Gynaecology (99.2%, n = 121) conducted more clean-contaminated procedures; while Dental (62.5%, n = 5) and Otorhinolaryngology (70.0%, n = 7) performed more clean procedures.
| Characteristic | Total sample (n=208) | Pre-operative Antibiotic Guideline Compliance | Post-operative Antibiotic Guideline Compliance | |||||
| N= 48 Frequency (%) | N=160 Frequency (%) | Association between patient/surgical characteristics and pre-operative guideline compliance P-value (CI 95%) | N= 35 Frequency (%) | N=173 Frequency (%) | ||||
| Frequency (%) | Median (IQR) | Compliant to Guideline | Non-compliant to Guideline | Compliant to Guideline | Non-compliant to Guideline | |||
| Age (years) | 32 (25-39.3) | |||||||
| Weight (kg) | 64.3 (55-74) | |||||||
| Gender | ||||||||
| Male | 61 (29.3%) | 35 (57.4%) | 26 (42.6%) | 11 (18.0%) | 50 (82.0%) | |||
| Female | 147 (70.7%) | 13 (8.8%) | 134 (91.2%) | 24 (16.3%) | 123 (83.7%) | |||
| Discipline | <0.001# | |||||||
| Surgical | 39 (18.8%) | 15 (38.5%) | 24 (61.5%) | 16 (41.0%) | 23 (59.0%) | |||
| Orthopedic | 29 (13.9%) | 21 (72.4%) | 8 (27.6%) | 5 (17.2%) | 24 (82.8%) | |||
| Obsterics & Gynaecology (O&G) | 122 (58.7%) | 2 (1.6%) | 120 (98.4%) | 14 (11.5%) | 108 (88.5%) | |||
| Dental | 8 (3.8%) | 0 (0.0%) | 8 (100%) | 0 (0.0%) | 8 (100.0%) | |||
| Otorhinolaryngology | 10 (4.8%) | 10 (100.0%) | 0 (0.0%) | 0 (0.0%) | 10 (100.0%) | |||
| Citizenship | 0.017$ | |||||||
| Local | 142 (68.3%) | 40 (28.2%) | 102 (71.8%) | 28 (19.7%) | 114 (80.3%) | |||
| Non-local | 66 (31.7%) | 8 (12.1%) | 58 (87.9%) | 7 (10.6%) | 59 (89.4%) | |||
| Time of Surgery | 0.586# | |||||||
| Initial | 203 (97.6%) | 48 (23.6%) | 155 (76.4%) | 34 (16.7%) | 169 (83.3%) | |||
| Subsequent | 5 (2.4%) | 0 (0.0%) | 5 (100.0%) | 1 (20.0%) | 4 (80.0%) | |||
| Type of Procedure | <0.001$ | |||||||
| Emergency | 117 (56.3%) | 12 (10.3%) | 105 (89.7%) | 10 (8.5%) | 107 (91.5%) | |||
| Elective | 91 (43.7%) | 36 (39.6%) | 55 (60.4%) | 25 (27.5%) | 66 (72.5%) | |||
| Wound Classification | <0.001$ | |||||||
| Clean | 42 (20.2%) | 23 (54.8%) | 19 (45.2%) | 17 (40.5%) | 25 (59.5%) | |||
| Clean-Contaminated | 166 (79.8%) | 25 (15.1%) | 141 (84.9%) | 18 (10.8%) | 148 (89.2%) | |||
| Prophylaxis Given > 24 hours | ||||||||
| Yes | 171 (82.2%) | |||||||
| No | 37 (17.8%) | |||||||
$ Chi Square Test; # Fisher Exact Test; IQR-interquartile range; CI-Confidence Interval
Pre-operative & Post-operative Antibiotic Prescribing
Table III presents the distribution of antibiotic groups prescribed during pre- and post- surgeries. The most commonly prescribed antibiotics for pre-operative prophylaxis were beta-lactam/beta-lactamase inhibitors (64.1%, n = 127), followed by cephalosporins (25.8%, n = 51), penicillin (5.6%, n = 11), and others (4.5%, n = 9).
The post-operative antibiotics administered closely mirrored those given pre-operatively, with beta-lactam/beta lactamase inhibitors (67.2%, n = 127) being the most frequently prescribed, followed by cephalosporins (20.1%, n = 38), other group (7.9%, n = 15), and penicillin (4.8%, n = 9).
Antibiotic Surgical Prophylaxis Guideline Compliance
Among the 208 cases, only 23.1% of the pre-operative cases (n = 48) complied with guidelines. Furthermore, 82.2% (n = 171) of the cases were given prophylactic antibiotics for more than 24 hours. Meanwhile, only 16.8% (n = 35) complied with the guideline recommendations for post-operative antibiotic use.
The study demonstrated no significant association between the time of surgery and pre-operative antibiotic guideline compliance. However, significant associations were observed between discipline, citizenship status, type of procedure, and wound classification.
Pre-operative antibiotic guideline compliance was significantly associated with the discipline variable (P < 0.001), with Dental (0%, n = 0) showing the lowest compliance rate, followed by Obstetrics and Gynaecology (1.6%, n = 2), Surgical (38.5%, n = 15), Orthopaedic (72.4%, n = 21) and Otorhinolaryngology (100.0%, n = 10).
A significant association was also observed between citizenship and pre-operative antibiotic prophylaxis guideline compliance (P = 0.017), with a lower rate of compliance cases among non-local patients (12.1%, n = 8). Both emergency procedures (10.3%, n = 12) and clean-contaminated surgeries (15.1%, n = 25) were significantly linked to lower rates of compliance with guidelines (P < 0.001).
Inappropriateness of Pre-operative Antibiotic Prophylaxis
There were 205 instances of inappropriateness identified in pre-operative antibiotic use, with the most common reason being incorrect dosing (59.0%), followed by incorrect antibiotics (12.2%) and incorrect timing (11.1%). Within each of the disciplines, the most common reasons for inappropriateness were found to be incorrect antibiotics for Surgical and Dental; incorrect dosing for Orthopaedic and Obstetrics & Gynecology.
Inappropriateness of Post-Operative Antibiotic Prophylaxis
There were 179 instances of inappropriateness detected in post-operative antibiotics use, with antibiotics not required (52.5%) reported as the most common reason, followed by incorrect duration (40.8%) and incorrect antibiotics (3.4%). Within each of the disciplines, the most common reasons for inappropriateness were reported to be antibiotics not required for Surgical and Otorhinolaryngology; incorrect duration for Orthopaedic and Obstetrics & Gynecology; and incorrect antibiotics for Dental.
DISCUSSION
Overall Compliance and Comparative Analysis
| Antibiotic Group | Pre-Operative Frequency (n) | Post-Operative Frequency (n) |
| Beta-lactams/Beta-lactamase Inhibitors | 127 (64.1%) | 127 (67.2%) |
| Cephalosporins | 51 (25.8%) | 38 (20.1%) |
| Penicillin | 11 (5.6%) | 15 (7.9%) |
| Others | 9 (4.5%) | 9 (4.8%) |
| Total | 198 (100.0%) | 189 (100.0%) |
Only 23.1% of the pre-operative cases showed appropriate antibiotic surgical prophylaxis use in this study. The appropriateness of surgical antibiotic prophylaxis was significantly associated with discipline, citizenship status, type of procedure, and wound classification.
The surgical chemoprophylaxis guideline compliance rate at Hospital Lahad Datu was found to be much lower compared to other studies carried out at Sarawak General Hospital (SGH) (70%, n = 87) [5], Universiti Kebangsaan Malaysia Medical Center (UKMMC) (75.21%, n = 121) [12), and Hospital Kuala Lumpur (HKL) (66%, n = 306) [4].
This study also demonstrated a high prevalence of prolonged antibiotic use beyond 24 hours post-operatively, with 82.2% of the cases receiving antibiotic prophylaxis for more than 24 hours. This contrasts with 23% at SGH (n = 87) [5], 33.2% at HKL (n = 419) [4], and 30.6% at Hospital Universiti Sains Malaysia (HUSM) (n = 216) [3]. Our findings are consistent with those from other international studies, which identified prolonged antibiotic prophylaxis use as the main reason for non-compliance [2,8,9,15].
Factors Influencing Guideline Compliance
Discipline was found significantly correlate with pre-operative antibiotics prophylaxis guideline adherence. This is similar to the study by Phan et al. in Vietnam, which showed a correlation between prophylactic antibiotic guideline compliance with supervision and inspection of prevention procedures within the department [14]. Otorhinolaryngology and Orthopaedics demonstrated high compliance, likely due to more standardised procedures and clearer prophylaxis protocols. In contrast, the Obstetrics & Gynecology department exhibited very low compliance (1.6%), reflecting conventional practices for surgical antibiotic prophylaxis based on older guidelines, especially for cases of caesarean sections. This may also be due to a lack of awareness of the latest NAG guidelines or a preference for senior-led practices. Focused antimicrobial stewardship (AMS) interventions and continuous professional education are therefore needed.
Pre-operative antibiotic prophylaxis guideline compliance was significantly associated with citizenship status. According to the 2020 Population and Housing Census conducted by the Department of Statistics Malaysia [13], Lahad Datu has a non-citizen population of 39.7%. Access to piped water, hospitals per 1,000 population, and health clinics per 1,000 population all fall below the national median in this constituency [13]. The majority of non-citizens or migrants in Sabah were employed in the plantation sector, and hence reside in rural plantations with suboptimal living conditions [16]. These conditions and limited access to public healthcare [17] may heavily influence a clinician’s decision-making regarding antibiotic use. In such settings, there may be a tendency to overtreat this category of patients to minimise the risk of surgical site infections (SSIs), particularly when post-discharge hygiene and follow-up care cannot be assured. Further studies are needed to explore the clinical decision-making process in such contexts. Regional studies have also reported that incomplete pre-operative documentation, varied referral pathways, and limited time for pre-surgical optimization contribute to poorer guideline compliance among non-local patients [18].
Similar to the findings by Phan et al. [14], the type of procedures significantly correlated with pre-operative antibiotic prophylaxis guideline compliance. Incomplete patient history taking and time constraints in carrying out emergency procedures have led to lower guideline compliance.
Wound classification was also found to be significantly associated with the appropriate use of pre-operative antibiotic prophylaxis. Studies have demonstrated that clean-contaminated wounds have a higher risk of infection compared to clean wounds [4,14]. The lack of confidence among clinicians regarding surgical outcomes or infection risks of clean-contaminated wounds may contribute to the lower guideline compliance rate in these cases. This ultimately results in the use of broader-spectrum antibiotics in clean-contaminated surgeries, as shown in our study.
Reasons for Inappropriate Prescribing Practices
The most commonly reported pre-operative reason for inappropriateness was incorrect dosing (59.0%, n = 121), where a lower (1.5g) than the recommended dose (3g) of IV Ampicillin/Sulbactam was prescribed for caesarean section cases, accounting for the majority of the cases. This finding suggests possible inconsistencies in guideline dissemination, limited familiarity with prophylactic dosing, or reliance on habitual dosing practices rather than updated evidence-based recommendations [19].
Incorrect pre-operative antibiotic selection (12.2%, n = 25) was also a contributing factor to non-compliance with guidelines. The results of our study are consistent with findings from other facilities in Malaysia, where antibiotic choice was one of the frequently encountered reasons for non-compliance [5,20]. Intravenous cefoperazone was used in cases of appendectomy instead of intravenous cefazolin or cefuroxime as recommended by the NAG. This deviation was likely attributable to established practice pattern driven by senior clinicians’ preferences, consistent with the findings of a study by Ali et al [15].
11.2% (n = 23) of the cases reported receiving antibiotic prophylaxis more than 60 minutes before surgery, causing incorrect timing of antibiotic administration, which is one of the leading causes of non-compliance. This finding is similar to the study conducted at HUSM (11.9%, n = 160) [3], while it showed a higher incidence compared to studies conducted at SGH (4.6%, n = 87) [5], UKMMC (6.7%, n = 163) [4] , and a multicentre study conducted in Selangor (7.6%, n = 120) [20]. Incorrect timing indicates workflow and coordination gaps within the peri-operative system. Timely administration, typically within 60 minutes prior to incision, is crucial for achieving optimal tissue concentrations at the start of surgery [21]. Deviations from the recommended timing window may stem from operating theatre delays, logistical challenges in patient transfer, or inadequate communication between operating theatre personnel. Strengthening perioperative coordination and standardizing antibiotic timing protocols could mitigate this issue [19]. Studies have shown a higher rate of SSIs in patients who received antibiotics at an inappropriate time compared to those who received antibiotics at the appropriate time [3,4].
Unnecessary use (52.5%, n = 94) and prolonged duration (40.8%, n = 73) of post-operative prophylactic antibiotics were the most frequent reasons for non-compliance in the post-operative stage. These findings are consistent with both local [3,5,20,22] and international studies [2,8,9,23]. Clinicians may extend the duration of post-operative antibiotic prophylaxis to mitigate the risk of SSIs, particularly in high-risk procedures or when post-operative monitoring is limited. This tendency toward defensive prescribing has been documented in qualitative studies and is often driven by concerns over adverse infection outcomes and medicolegal liability [15]. However, prolonged prophylactic antibiotic use has not been shown to significantly improve SSI outcomes [3,23] and is associated with additional costs [22] and an increased risk of antibiotic resistance. Notably, lower compliance among non-local patients may be influenced by suboptimal living conditions, which in turn can affect clinicians’ prescribing decisions. In such contexts, clinicians may extend antibiotic use post-operatively to reduce the risk of SSIs, particularly when post-discharge hygiene and follow-up care are uncertain.
Targeted Antimicrobial Stewardship (AMS) Interventions
To address the findings of this study, AMS interventions are urgently needed at the hospital level. A focused educational programme should be implemented to address the most common pre-operative prescribing errors, particularly the incorrect dosing of intravenous ampicillin/sulbactam in caesarean sections and the inappropriate selection of antibiotics for appendectomy procedures.
To mitigate incorrect antibiotic administration timing driven by peri-operative workflow delays, the standardisation of operating theatre protocols is essential. The implementation of clinical decision support tools, such as checklist-based or electronic reminder systems, alongside strengthened multidisciplinary collaboration among operating theatre personnel, is recommended to ensure administration occurs within the optimal 60-minute pre-incision window.
Furthermore, regular audits coupled with targeted feedback are essential to reduce the prevailing reliance on defensive prescribing practices. These audits should specifically support clinicians in confidently discontinuing post-operative antibiotics within 24 hours for clean-contaminated wounds, while also providing evidence-based reassurance for the management of patients from rural and non-citizen populations, where concerns regarding post-discharge hygiene and follow-up care may influence prescribing behaviour.
Limitations
Several limitations were identified in our study. First, the universal sampling method used resulted in participants not being randomly chosen, leading to over- or under-representation of certain groups due to uneven distribution among the groups. This imbalance may have reduced statistical power and limited the feasibility of multivariable analysis due to insufficient variability in key categorical variables. Although multivariable logistic regression could provide adjustment for potential confounders, the unequal distribution of cases across several categories and limited variability within some study groups reduced the robustness of multivariable modelling. Therefore, the analysis was restricted to univariate methods and findings should be interpreted as exploratory associations rather than independent predictors.
Second, this is a single-centre study, meaning the findings cannot be generalised to the broader population, hence limiting external validity. Third, the observational design does not allow for the establishment of causal relationships between the identified factors and guideline compliance.
Fourth, as only univariate analyses were performed, potential confounding factors could not be controlled. Therefore, observed associations may be influenced by other clinical or procedural variables not accounted for in the analysis.
Fifth, data collection relied on documentation in medical records and medication charts; therefore, incomplete or inaccurate documentation may have resulted in misclassification of compliance and appropriateness assessments.
Sixth, as data were collected prospectively, a potential Hawthorne effect may have influenced prescribing behaviour, whereby clinicians may have modified their practice due to awareness of being observed.
Seventh, the study did not evaluate surgical site infection outcomes; therefore, the relationship between guideline compliance and clinical outcomes could not be determined. Despite these limitations, this study provides valuable insight into current surgical antibiotic prophylaxis practices and identifies important targets for future antimicrobial stewardship interventions and quality improvement initiatives
| Discipline | Reason of Inappropriateness n, (%) | |||||||||
| Incorrect Antibiotics | Incorrect Dose | Incorrect Timing | Spectrum Too Broad | Spectrum Too Narrow | Spectrum Overlapping | Antibiotic Required but Not Given | Antibiotic Not Required | Repeated Antibiotic Required, but Not Given | TOTAL | |
| Surgical | 13 (29.6%) | 4 (9.1%) | 6 (13.6%) | 11 (25.0%) | 2 (4.5%) | 0 (0.0%) | 2 (4.5%) | 5 (11.4%) | 1 (2.3%) | 44 (100.0%) |
| Orthopedic | 1 (11.1%) | 3 (33.4%) | 0 (0.0%) | 1 (11.1%) | 0 (0.0%) | 0 (0.0%) | 2 (22.2%) | 2 (22.2%) | 0 (0.0%) | 9 (100.0%) |
| Obstetrics & Gynaecology | 6 (4.3%) | 114 (82.0%) | 17 (12.3%) | 0 (0.0%) | 2 (1.4%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 139 (100.0%) |
| Dental | 5 (38.5%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 5 (38.5%) | 0 (0.0%) | 1 (7.7%) | 1 (7.7%) | 1 (7.7%) | 13 (100.0%) |
| Otorhinolaryngology | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) |
| Total | 25 (12.2%) | 121 (59.0%) | 23 (11.2%) | 12 (5.9%) | 9 (4.4%) | 0 (0.0%) | 5 (2.4%) | 8 (3.9%) | 2 (1.0%) | 205 (100.0%) |
CONCLUSION
This study shows a low compliance rate (23.1%) with surgical antibiotic prophylaxis guidelines at Hospital Lahad Datu, with compliance significantly associated with surgical discipline, patient citizenship, wound classification, and type of procedure. The most common errors driving this non-compliance were incorrect pre-operative dosing and unnecessarily extending post-operative antibiotics beyond 24 hours. To improve adherence and reduce inappropriate antibiotic use, targeted Antimicrobial Stewardship (AMS) interventions should be implemented. Key recommendations for hospital policy include targeted education to correct specific prescribing habits such as the incorrect dosing for caesarean sections and improper antibiotic selection for appendectomies, as well as the use of standardised workflows with checklists or electronic reminders to ensure antibiotics are administered exactly within the 60-minute pre-incision window. Furthermore, conducting regular audits with targeted feedback is essential to actively discourage defensive prescribing, which will help clinicians confidently stop post-operative antibiotics within 24 hours. Future research should include surgical site infections as outcome measures to correlate antibiotic guideline compliance for a better understanding, as well as improvement of future practice and consider broader sampling across multiple centres. A follow-up audit is also recommended after the interventions have been conducted to evaluate the impact of these interventions on antibiotic prophylaxis compliance.
ACKNOWLEDGEMENT
We would like to thank the Director General of Health Malaysia for permission to publish this paper. We would also like to expand our appreciation to all healthcare providers and colleagues who contributed to and assisted with data collection, data analysis, interpretation, as well as manuscript writing for this study.
CONFLICT OF INTEREST
All the investigators in this study declared no conflict of interest. This study did not receive funding from any public, private, or non-profit agency.
REFERENCE
- Centers for Disease Control and Prevention. National Healthcare Safety Network (NHSN) patient safety component manual. 2024.
- Vazin A, Hatami-Mazinani N, Alemzadeh E, Dehghani F, Mahi-Birjand M. Compliance with antibiotics prophylaxis guideline in surgical patients in ICUs of a teaching referral hospital. Health Serv Insights 2022; 15: 11786329221136437. https://doi.org/10.1177/11786329221136437
- Khan OH, Zakaria AD, Hashim MN, Khan AH, AlQarni A, AlGethamy M, et al. The burden of surgical site infection at Hospital Universiti Sains Malaysia and related postoperative outcomes: a prospective surveillance study. Antibiotics (Basel) 2023; 12(2): 208. https://doi.org/10.3390/antibiotics12020208
- Fadzwani B, Raha AR, Nadia MN, Wan Rahiza WM, Razman J, Nordiah AJ. Surgical antibiotic prophylaxis: incidence and risk of surgical site infection. IIUM Med J Malaysia 2020; 19(1): 45–53. https://doi.org/10.31436/imjm.v19i1.1331
- Oh AL, Goh LM, Nik Azim NA, Tee CS, Phung Shehab CW. Antibiotic usage in surgical prophylaxis: a prospective surveillance of surgical wards at a tertiary hospital in Malaysia. J Infect Dev Ctries 2014; 8(2): 193–201. https://doi.org/10.3855/jidc.3076
- Allegranzi B, Bischoff P, de Jonge S, Kubilay NZ, Zayed B, Gomes SM, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis 2016; 16(12): e276–e287. https://doi.org/10.1016/S1473-3099(16)30398-X
- Ban KA, Minei JP, Laronga C, Harbrecht BG, Jensen EH, Fry DE, et al. American College of Surgeons and Surgical Infection Society: surgical site infection guidelines, 2016 update. J Am Coll Surg 2017; 224(1): 59–74. https://doi.org/10.1016/j.jamcollsurg.2016.10.029
- Ahmed N, Balaha M, Haseeb A, Khan A. Antibiotic usage in surgical prophylaxis: a retrospective study in the surgical ward of a governmental hospital in Riyadh region. Healthcare (Basel) 2022; 10(2): 387. https://doi.org/10.3390/healthcare10020387
- Ierano C, Thursky K, Marshall C, Koning S, James R, Johnson S, et al. Appropriateness of surgical antimicrobial prophylaxis practices in Australia. JAMA Netw Open 2019; 2(11): e1915003. https://doi.org/10.1001/jamanetworkopen.2019.15003
- Berríos-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, et al. Centers for Disease Control and Prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg 2017; 152(8): 784–791. https://doi.org/10.1001/jamasurg.2017.0904
- Ministry of Health Malaysia. National antimicrobial guideline (NAG) 2024. 4th ed. Pharmaceutical Services Programme, Ministry of Health Malaysia 2024.
- Dyar OJ, Huttner B, Schouten J, Pulcini C. What is antimicrobial stewardship? Clin Microbiol Infect 2017; 23(11): 793–798. https://doi.org/10.1016/j.cmi.2017.08.026
- Department of Statistics Malaysia. Subnational statistics parliament and state legislative assembly: P.188 Lahad Datu, Sabah. Putrajaya: Department of Statistics Malaysia 2022.
- Van Tuong P, Xiem CH, Anh NC, Quang LN. Assessment of antibiotic prophylaxis in surgical patients and association factors at Thu Duc District Hospital, Ho Chi Minh City, Vietnam in 2018. Health Serv Insights 2021; 14: 11786329211029354. https://doi.org/10.1177/11786329211029354
- Ali N, Hamouda R, Tarek R, Abdelhamid M, Lashin A, Hassan R, et al. Non-adherence to surgical antibiotic prophylaxis guidelines: findings from a mixed-methods study in a developing country. Antimicrob Resist Infect Control 2025; 14: 89. https://doi.org/10.1186/s13756-025-01607-5
- Sayed Mahadi SAR, Hussin H, Khoso A. Linkages between income resources, the cost of living and the remittance: case of Indonesian migrant workers in Sabah Malaysia. Borneo Res J 2017; 11(1): 1–28. https://doi.org/10.22452/brj.vol11no1.1
- Loganathan T, Rui D, Ng CW, Pocock NS. Breaking down the barriers: understanding migrant workers’ access to healthcare in Malaysia. PLoS One 2019; 14(7): e0218669. https://doi.org/10.1371/journal.pone.0218669
- Farasatinasab M, La’li A, Zibafard A, Khaleghian M, Nasiripour S, Alizadeh Otaghvar H, et al. Evaluation of surgical antibiotic prophylaxis guideline adherence: a cross-sectional study of two Iranian teaching hospitals. Arch Clin Infect Dis 2025; 20(2): e148269. https://doi.org/10.5812/archcid-148269
- Gouvêa M, Novaes CO, Pereira DMT, Iglesias AC. Adherence to guidelines for surgical antibiotic prophylaxis: a review. Braz J Infect Dis 2015; 19(5): 517–524. https://doi.org/10.1016/j.bjid.2015.06.004
- Pang CW, Shaik Ismail SM, Adnan S, Sim B. Improving perioperative antibiotic administration using PDSA cycles: a Selangor state surgical prophylaxis audit. Int J Infect Dis 2020; 101(Suppl 1): 100. https://doi.org/10.1016/j.ijid.2020.09.283
- Bratzler DW, Dellinger EP, Olsen KM, Perl TM, Auwaerter PG, Bolon MK, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm 2013; 70(3): 195–283. https://doi.org/10.2146/ajhp120568
- Gul YA, Hong LC, Prasannan S. Appropriate antibiotic administration in elective surgical procedures: still missing the message. Asian J Surg 2005; 28(2): 104–108. https://doi.org/10.1016/S1015-9584(09)60272-4
- Thabit AK, Fairaq EM, Almutairi FS. Appropriateness of choice and duration of surgical antibiotic prophylaxis and the incidence of surgical site infections: a prospective study. J Taibah Univ Med Sci 2023; 18(1): 26–31. https://doi.org/10.1016/j.jtumed.2022.08.012
Please cite this article as:
Thiban Ellumalay, Sim Pei Fren, Phua Sook Hui, Muhammad Firdaus Bin Mohd Nor, Darren Stacey Simon, Siti Sarah Binti Mat Saad, Tan Tiong Herng, Tan Pei Kheng, Erra Fazira Binti Ahmad and Sithtarrthen K. Arumugam, Guideline Compliance and Determinants of Inappropriate Surgical Antibiotic Prophylaxis in a District Hospital in Sabah: A Prospective Audit. Malaysian Journal of Pharmacy (MJP). 2026;2(12):59-68. https://mjpharm.org/guideline-compliance-and-determinants-of-inappropriate-surgical-antibiotic-prophylaxis-in-a-district-hospital-in-sabah-a-prospective-audit/