Introduction
Chronic kidney disease (CKD) is a major global health issue, particularly in resource-constrained nations [1]. It is a progressive condition that can cause kidney failure and necessitate renal replacement treatment, and it is associated with morbidity and mortality at all stages [2]. The economic, clinical, and humanistic consequences are tremendous [3]. Fortunately, medicines exist to decrease disease consequences [4], as well as to delay or even stop progression to severe stages [5]. Almost all medications are aiming at preventing renal disease progression and minimizing related consequences, on the other
hand, relying mainly on patient self-care. Throughout the various stages of CKD, patients with CKD need to invest considerable time into managing their health, including modifying their diet and lifestyle, managing numerous medications, and attending medical appointments. Therefore, knowledge of the disease and its management is required for the effective management of CKD at home by patients. As a result of the disease’s complexity, which necessitates patients’ active participation and the acquisition of self-management skills, medical education is crucial in the CKD population [6]. Therefore, insufficient medical education is a major issue in many chronic diseases, including CKD. Chronically ill people with low medical education have little understanding of their medical condition or how to manage it [7].
Evidence suggests that the general population, as well as CKD patients, have a lack of knowledge about the disease. Most people in the general population lack knowledge of their kidney disease [8]. The worst of it all is that most patients with CKD who are being managed by experts have limited knowledge of the disease [9]. A study revealed that a considerable proportion of patients with CKD stages 3 – 5 have poor knowledge about their own CKD diagnosis, and what to do if their kidneys fail [9]. Furthermore, studies consistently demonstrate that patients need more knowledge about their chronic medical conditions to promote self-care behaviors [10-14] and that a lack of effective communication from health professionals is perceived as a constraint to acquiring and comprehending this information [15].
The provision of CKD-specific knowledge interventions, such as knowledge of kidney physiology, functions, causes of CKD, symptoms, diagnosis, the importance of dietary and lifestyle modifications, and adherence to medication, control of co-morbidities to slow down disease progression among others is critical since educational interventions have been found to postpone the start of dialysis and lower the risk of death due to CKD [16]. There is, however, a scarcity of data on educational programmes for the CKD population in low- and middle-income countries (LMICs), including Nigeria. As a result, the aims of the study were to determine the impact of pharmacists’ educational interventions on the CKD knowledge and knowledge levels of patients with pre-dialysis CKD and to identify potential predictors of good CKD knowledge.
Method
Study Design and Setting
This was a randomised, controlled, prospective study with a 12-month follow-up. The study was conducted from November 2019 to October 2020 in two main healthcare facilities in Maiduguri, Nigeria.
Sample Size Calculation
An online Sealed Envelope® sample size calculator was used to calculate the required sample size [17]. This study was powered at 90% (2-sided test level of 0.05) to detect a difference in the mean overall knowledge scores at 6 and 12 months between the 35 percent receiving usual care and the 65 percent receiving the intervention. The sample size required for each group was 54 people. The minimal sample size of 108 was increased to account for an anticipated 7% noncompliance in both groups, yielding a final value of 148.
Calculation is based on the formula:
n = f (α/2, β) × [p1 × (100 − p1) + p2 × (100 − p2)] / (p2 − p1)2
Where p1 and p2 are the percent ‘success’ in the control and experimental group respectively, and
f (α, β) = [Φ-1(α) + Φ-1(β)]2
Φ-1 is the cumulative distribution function of a standardised normal deviate.
Adjustment for non-compliance is based on formula:
nadj = n × 10,000 / (100 – c1 – c2)2
Where c1 and c2 are the percent non-compliance in the control and experimental group respectively.
Eligibility Criteria
Patients that were 18 to 85 years old with a confirmed CKD stage 1 – 4 diagnosis who consented, stated readiness to abide by the study protocols, and expressed a willingness to remain in Maiduguri throughout the study period were enrolled. Patients with acute renal failure (ARF), eligible individuals who refused to sign informed consent, and those at CKD stage 5 were excluded. Pregnant or lactating women, patients on dialysis or post-renal transplant patients, patients with HIV infection, critically sick patients or patients known to have current psychosis, dementia, or cognitive impairment, and those who expressed a readiness to withdraw from the study were also excluded.
Ethical Considerations
Ethical approvals were provided by the Research Ethics Committees of the study healthcare facilities. All participants who volunteered to take part in this study provided written informed consent. The confidentiality of patients’ information was upheld throughout the study period. During data collection, codes were used to identify participants.
Participants Selection, Randomisation, and Stratification
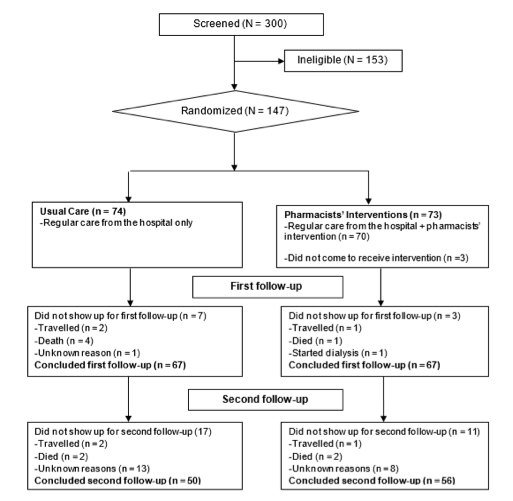
In order to identify those eligible for the study the health information of patients with CKD was reviewed in the clinic using screening and eligibility forms. The patients who had been identified were approached and invited to participate utilising the consent explanation forms. The consent declaration form was signed by all who volunteered to be included in the trial. Participants were randomised in a 1:1 ratio to the Usual Care (UC) and Pharmacists’ Intervention (PI) groups (Figure 1) using computer-generated random numbers stratified by CKD stage [18].
Usual Care Received
The usual/conventional care provided to the UC group by the hospitals, included hospital visits for follow-up or due to new sickness, physician consultations, regular medical investigations, review of diagnosis, medications, and referral when necessary. The usual care was provided with no teachings/coaching about their medical conditions or medicines and with no patient empowerment to fully participate in self-management techniques.
Interventions
For 12 months, participants in the PI group got usual care as well as pharmacists’ interventions provided by three final-year pharmacy students trained by the authors. The PI group received usual care and face-to-face CKD education at baseline (group education), 6 months, and 12 months (individualised according to each patient’s needs), as well as educational infographics on CKD at baseline. The structured education programme for patients in the intervention group consisted of five sessions of 90 – 120 minutes each covering the physiology of kidneys and six kidney disease education lessons [19]: (i) Comprehending renal disease, (ii) Renal disease management, (iii) Manifestations of worsening renal disease, (iv) Treatment choices for renal failure, (v) Preparations for renal failure treatments, and (vi) Living with renal failure. The structured sessions were conducted once at baseline in groups of 4 to 10 patients after data collection. Additionally, throughout the study period, cell phone CKD educational text messages based on the topics covered during the baseline face-to-face education were provided to each patient fortnightly, while participants phoned-in when the need arises, Reinforcement interventions through phone calls were also provided on individual needs basis.
Blinding
The profession of the investigators was not made known to the participants to rule out potential sources of bias because pharmacists are seen mainly by patients as drug dispensers in Nigeria.
Follow-Up Visits
At six and 12 months, all participants returned to the research clinic for follow-ups. The same instrument was used to conduct an additional CKD knowledge assessment and reinforcing interventions according to each participant’s needs were also provided.
Study Outcomes
The primary outcome of the study was a change in the mean knowledge scores between the baseline and the first and second follow-ups, respectively. The secondary outcomes were the proportion of participants with correct knowledge of CKD at six and 12 months, respectively, and the potential predictors of good CKD knowledge at 12 months.
Variables Definition
Chronic kidney disease was defined as reduced kidney function (eGFR < 60 mL / min / 1.73m2) and / or the presence of markers of kidney damage for a period exceeding three months [20].
Study Instrument
A previously validated Kidney Disease Knowledge Survey (KiKS) questionnaire was used in this study [21]. This tool was updated by the authors of the present study to improve the participants’ understanding and facilitate filling. The “don’t know” option was added to help collect the correct responses that best describe an individual., Tylenol was replaced with paracetamol, which is the name used in Nigeria. To ensure the validity of the instrument in our study population, face validity was checked by four experts in CKD (two nephrologists and consultant renal pharmacists each). Based on their feedback, all the 28 items were kept without revision. Furthermore, a pilot study was conducted using the updated questionnaire on 20 patients with CKD that were excluded from the main study. The updated questionnaire had Cronbach’s alpha values of 0.71 for general knowledge, 0.64 for kidney functions, and 0.67 for CKD symptoms of progression respectively, indicating acceptable reliability scores.
The KiKS assesses CKD-specific knowledge in patients with CKD (stages 1 – 5) to better ascertain their degree of comprehension. The questions focus on knowledge of renal function, therapeutic options for renal failure, signs, and symptoms of disease progression, potentially beneficial or toxic medications, blood pressure targets, and other important topics to preserve kidney function. There are 28 questions in all, five of which are multiple-choice and 23 of which are yes/no/don’t know. The 28 questions are organised into three domains, namely: (i) General knowledge (9 questions), (ii) Knowledge of kidney functions (9 questions), and (iii) Knowledge of symptoms of progression of CKD or failure (10 questions). The sum of all the 28 questions constituted the total knowledge.
Data Collection
Participants’ relevant demographics were gathered at the baseline. Comorbidities were extracted from the patients’ medical records, while self-reported CKD knowledge information was gathered during each research visit.
Data Processing
Glomerular filtration rate (GFR) based on the Modification of Diet in Renal Disease Equation for Adult was used for disease staging [22][23]. To determine the CKD knowledge level, each correct answer was assigned one point, while zero points were assigned to each incorrect or don’t know answer. The overall knowledge score is the total of the correct answers to each question, ranging from 0 to 28 points, where 28 points indicate the highest level of knowledge. The overall knowledge was categorised, using Bloom’s cut-off point, as high if the score is between 80 and 100% (22 – 28 points), moderate if the score is between 60 and 79% (17 – 21 points), and low if the score is less than 60% (< 17 points) [24]. For the multivariable logistic regression analysis, good CKD knowledge was coded one, while sub-optimal CKD knowledge (low and moderate knowledge) was coded zero.
Data Analysis
In the analysis of the study data, per protocol procedure was used. Continuous data were summarised using their mean ± standard deviation (SD), while categorical variables were represented by crude counts and percentages. Proportions were compared with chi-square or fisher’s exact tests (when more than 20 percent of cells have expected frequencies of less than five). The independent samples t-test was used to compare the mean values of the study groups. The multivariable logistic regression analysis was performed at the end of the study to identify the potential predictors of good CKD knowledge among the study participants. In all analyses, p-values less than 0.05 were considered statistically significant (2-sided). SPSS for Windows version 21 was used for all analyses.
Result
The UC group received 74 (50.3%) of the 147 eligible and recruited participants, whereas the PI group received 73 (49.7%). Sixty-seven (90.5%) participants in the UC group and 67 (91.8%) in the PI group visited the research clinic during the
6 months follow-up, and their data were examined. Furthermore, 50 (67.6%) participants in the UC group and 56 (76.7%) in the PI groups completed the last follow-up, and only their data were included in the analysis at this timepoint (Figure I).
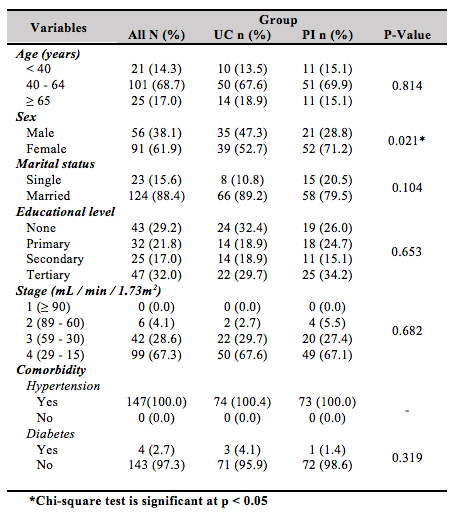
PI and UC groups had average age values of 51.1 (13.4) years and 53.3 (12.1) years, respectively. Overall, the baseline data of the study groups were similar, although the PI group had more females with a significant difference (71.2% vs. 52.7%, p = 0.021). The detailed baseline information of the participants is presented in Table I.
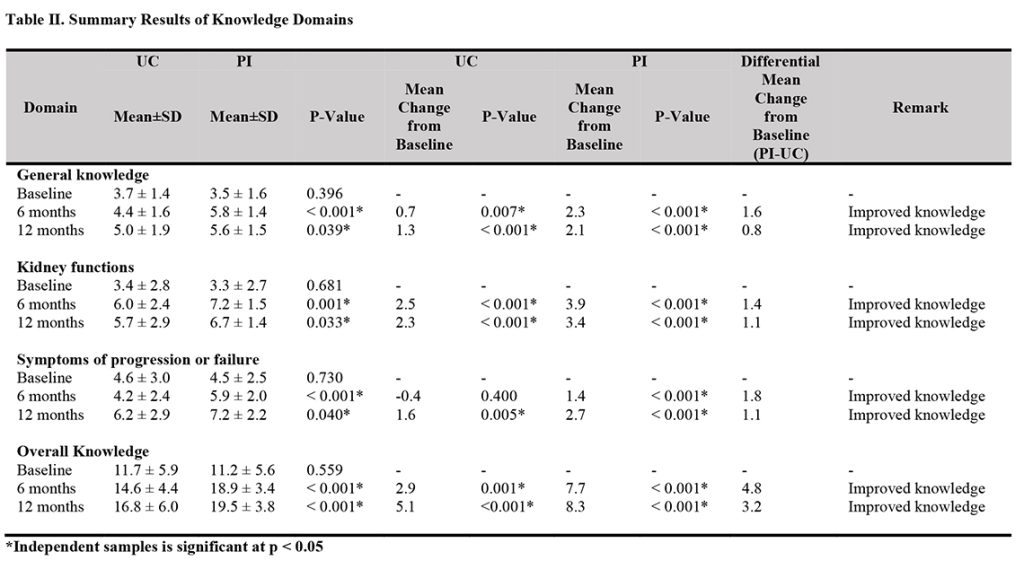
The mean general knowledge score of the PI group was significantly higher than that of the UC group at six months (5.8 ± 1.4 vs. 4.4 ± 1.6, p < 0.001), and at 12 months (5.6 ± 1.5 vs. 5.0 ± 1.9, p = 0.039). The mean kidney functions knowledge score of the PI group was significantly higher than that of the UC group at six months (7.2 ± 1.5 vs. 6.0 ± 2.4, p = 0.001), and at 12 months (6.7 ± 1.4 vs. 5.7 ± 2.9, p = 0.033). Also, the mean CKD symptoms of progression or failure knowledge of the PI group was significantly higher than that of the UC group at six months (5.9 ± 2.0 vs. 4.2 ± 2.4, p < 0.001), and at 12 months (7.2 ± 2.2 vs. 6.2 ± 2.9, p = 0.040). Further, the mean overall knowledge of the PI group was significantly higher compared with the UC group at six months (18.9 ± 3.4 vs.14.6 ± 4.4, p < 0.001), and at 12 months (19.5 ± 3.8 vs.16.8 ± 6.0, p < 0.001), respectively (Table II).
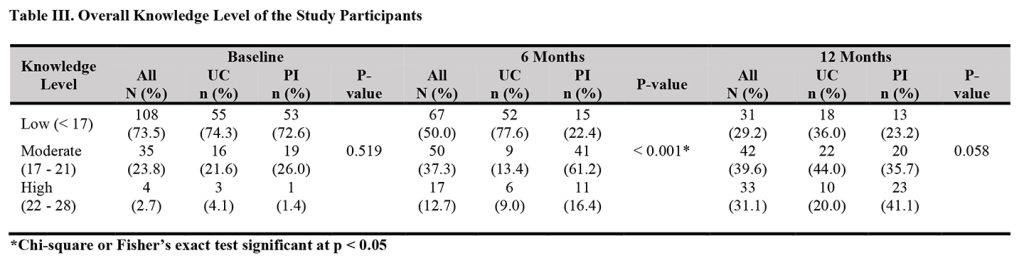
The overall CKD knowledge level was generally low (73.5%) in both groups at baseline with no statistically significant difference between the two study groups (72.6% in the PI vs. 74.3% in the UC, p = 0.519). At six months, a significant proportion of the participants in the intervention group had high knowledge compared with those in the UC group (16.4% vs. 9.0%, p < 0.001). Also, at 12 months, a higher proportion of participants in the intervention group had high knowledge compared with those in the UC group, although no statistically significant level was reached (41.1% vs. 20.0%, p = 0.058). The detailed distribution of the study participants based on their overall knowledge levels is presented in Table III.
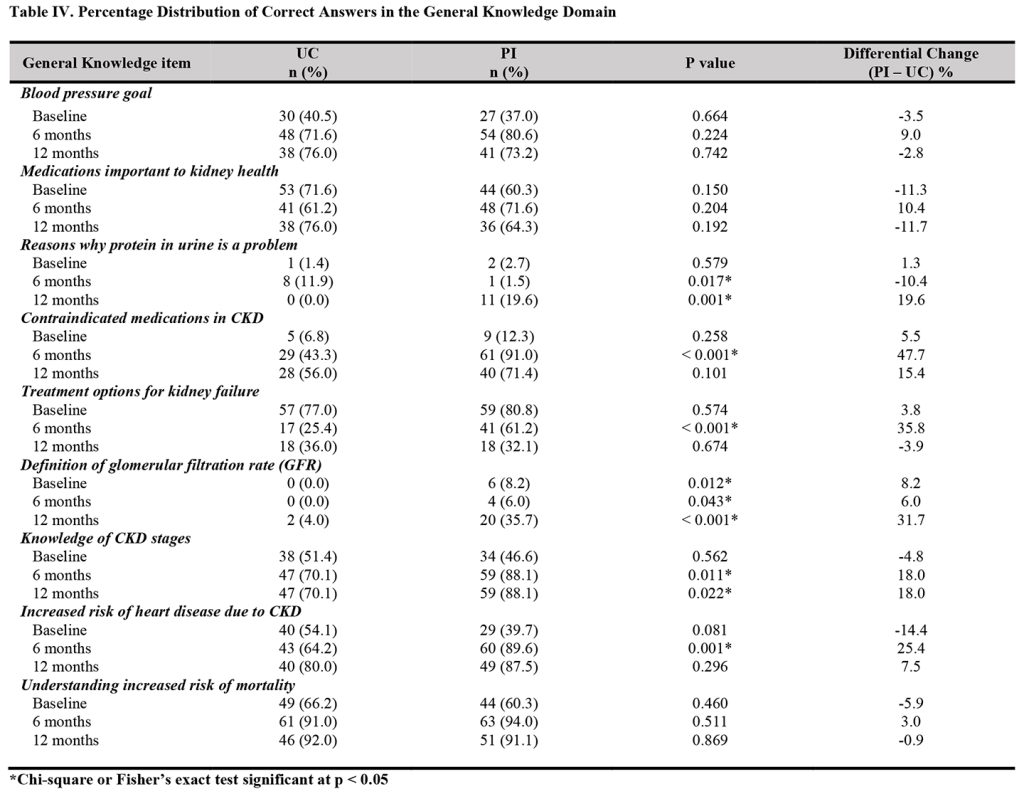
The analysis of the individual items of the general knowledge domain revealed a significantly higher proportion of participants in the intervention group than in the UC group that had correct knowledge of the reasons why protein in urine is a problem at the end of the study (19.6% vs. 0.0%, p = 0.001), medications a person with CKD should avoid (91.0% vs. 43.3%, p < 0.001]), and treatment options for kidney failure at six months (61.2% vs. 25.4%, p < 0.001). Also, a significantly higher proportion of participants in the intervention group than in the UC group had correct knowledge about the definition of glomerular filtration rate (GFR) at the baseline (8.2% vs. 0.0%, p = 0.012), six months (6.0% vs. 0.0%, p = 0.043), and 12 months (35.7% vs. 4.0%, p < 0.001). Further, a significantly higher proportion of participants in the intervention group than
in the UC group that had correct knowledge of stages of CKD at six months (88.1% vs. 70.1%, p = 0.011) and 12 months (88.1% vs. 70.1%, p = 0.022), and increased risk of heart disease at six months (89.6% vs. 64.2%, p = 0.001) (Table IV).
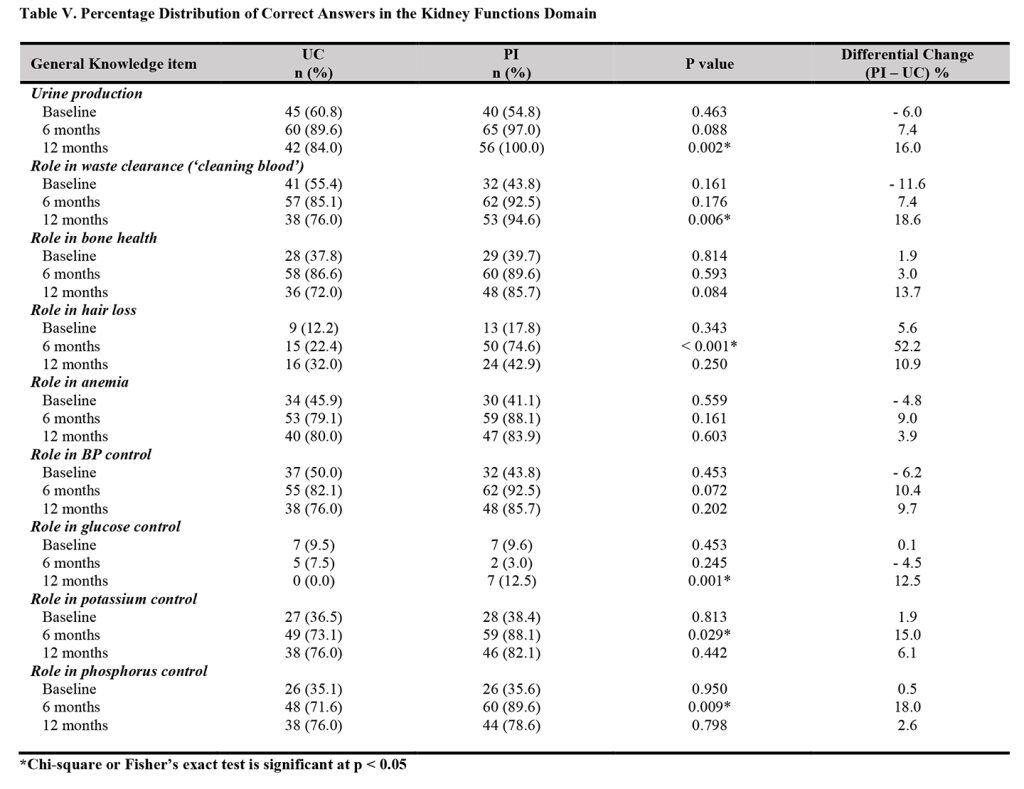
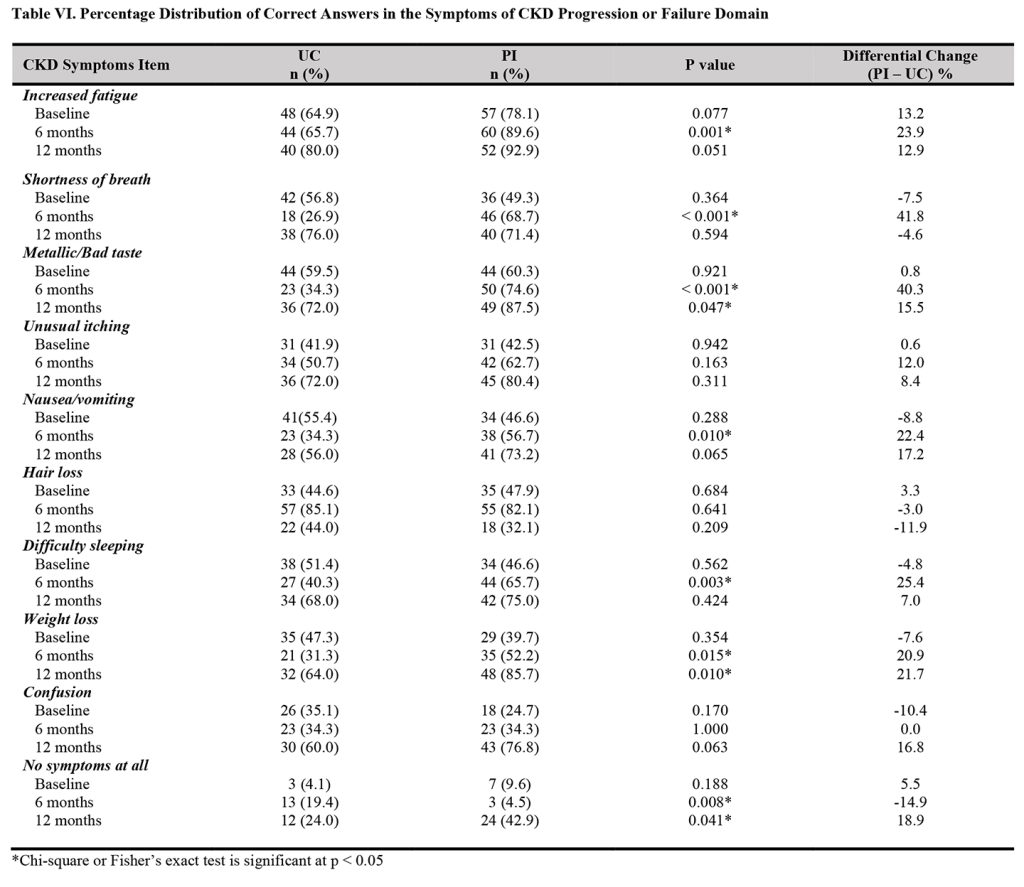
The analysis of the individual items of the kidney functions domain indicated that interventions provided by pharmacists led to significantly higher proportions of participants with correct knowledge of the roles of the kidneys in urine production at 12 months (100.0% in the PI vs. 84.0% in the UC, p = 0.002), the role in waste clearance at 12 months (94.6% in the PI vs. 76.0% in the UC, p = 0.006), and no hair loss role at six months (74.6% in the PI vs. 22.4% in the UC, p < 0.001). Also, significantly higher proportions of participants in the” intervention group than in the UC had correct knowledge about no glucose control role of kidney at 12 months (12.5% vs. 0.0%, p = 0.001), the role in potassium control at six months (88.1% vs. 73.1%, p = 0.029), and the role in phosphorus control at six months (89.6% vs. 71.6%, p = 0.009) (Table V). Also, the analysis of the individual items in the symptoms of progression or failure domain revealed significantly higher proportion of participants in the intervention group than in the UC group with correct knowledge of symptom of increased fatigue at 6 months (89.6% vs. 65.7%, p = 0.001), shortness of breath at six months (68.7% vs. 26.9%, p < 0.001), and metallic/bad taste at six months (74.6% vs. 34.3%, p < 0.001), and 12 months (87.5% vs. 72.0, p = 0.047). Further, significantly higher proportions of participants in the intervention group compared with the control group had correct knowledge about nausea/vomiting symptom at six months (56.7% vs. 34.3%, p = 0.010), difficulty sleeping at six months (65.7% vs. 40.3%, p = 0.003, weight loss at six months (52.2% vs. 31.3%, p = 0.015, and 12 months (85.7% vs. 64.0%, p = 0.010), and no symptoms at all at 12 months (42.9% vs. 24.0%, p = 0.041) (Table VI).
The multivariate logistic analysis using only the participants that completed the study revealed that patients between 40 and 64 years of age (AOR 26.3, 95% CI 2.1 – 331.0) and 65 years or more (AOR 10.1, 95% CI 1.1 – 89.7) had significantly higher odds of having good CKD knowledge compared to younger ones. Also, patients in the intervention group (AOR 2.7, 95% CI 1.0 – 7.2) had a significantly higher odds of having good CKD knowledge compared to those in the UC group, as shown in Table VII.
DISCUSSION
To the best of our knowledge, this is the first study to assess the efficacy of pharmacist-led educational interventions in a CKD
population in Africa. Our study found that the intervention group had a significantly larger proportion of participants who had correct information about kidneys and CKD than the control group. Overall, knowledge of CKD improved significantly in the intervention group compared to the control
group at six months. Also, a significantly higher proportion of participants in the intervention group had good knowledge of CKD compared to those in the control group at six months.
In our study, pharmacists’ interventions resulted in significantly greater proportions of participants who had correct knowledge about kidneys and CKD. Given the limited CKD knowledge among patients with CKD [9], and the increasing prevalence of kidney failure [25], it is imperative to improve CKD knowledge and its management to help improve self-management practices capable of retarding or halting the progression to renal failure. Available evidence has shown that educational interventions enhance outcomes in other chronic diseases such as heart failure [26], diabetes [27], and chronic obstructive pulmonary disease [28]. Overall, there was improved knowledge of CKD in the intervention group compared with the usual care group during the study period. In agreement with our result, an India-based non-randomised and non-controlled study of 69 patients with CKD over six months duration that evaluated pharmacists’ interventions also observed significantly improved knowledge of CKD among the participants at the end of the study [29]. In this study, pharmacists educated and counselled patients with CKD by utilising patient information leaflets, while follow-up was done bi-monthly for a period of six months. A study that evaluated the impact of pharmaceutical care among 120 patients with pre-dialysis CKD in Pakistan also noted significant knowledge improvement in the intervention group at the end of three months follow-up period [30].
In this study, pharmacists’ interventions included the provision of information on the disease, proper diets, counselling to enhance medication adherence, and follow-up through the telephone. Additionally, the result of our study is comparable with that of a non-randomised controlled multi-healthcare professional collaborative interventional study conducted in Korea among patients with pre-dialysis CKD, which reported a significant improvement in CKD knowledge scores over time in the intervention group compared to the control group [31]. In this study, CKD specialists (physicians, nurses, and nutritionists) offered interventions such as face-to-face group education and individualised consultation, re-inforcement education, and consultation to build up patients’ self-management skills to retard disease progression. Another study done in Korea that included patients undergoing early haemodialysis noted that educational interventions resulted in improved knowledge of patients [32]. Further, a prospective, pre–post study that enrolled 64 patients with dialysis CKD in Nepal also reported improved knowledge after pharmacist-provided counselling intervention [33]. Despite, the shorter duration of some of these previous studies, in the absence of additional important healthcare professionals required for renal care in the study settings, these findings may suggest a communication gap between patient and physician. As a result, there is a greater need for a shift in educational tactics, as well as the deployment of extra resources and appropriate healthcare professionals to help facilitate kidney disease education for patients. Regarding the additional healthcare professionals required, a multidisciplinary renal care team that includes a clinical pharmacist and other relevant healthcare professionals is critical to optimising health outcomes in CKD. The importance of pharmacists in providing patients with information on blood pressure monitoring, cardiovascular risk minimization, medication dose adjustment, and information on renally-eliminated medications, and anaemia management in renal diseases cannot be overstated. This is evidenced by a considerably higher proportion of participants in our study’s intervention group who knew about contraindicated medications or those to be used with caution in renal disease during the 12-month trial period. Available evidence demonstrates that increased disease-specific knowledge results in an enhanced personal-care practices [29].

Furthermore, the current pharmacist education programme could expand opportunities for direct connections between CKD patients and other important renal care professionals. Conversely, no significant improvement in knowledge of kidney function in the intervention group was observed in the Korean study [29]. This finding suggests a potential gap in the understanding of kidney functions by the participants of this study despite educational interventions provided by multi-healthcare professionals. Also, contrary to our results, a pre-and post-study that involved allied health staff or CKD nurse educators’ CKD educational interventions in Australia reported a minor improvement in patients’ knowledge of kidney disease at 12.7 months [34]. Variations in methods, healthcare professionals, and interventions involved could account for the observed differences.
Pharmacists’ intervention as a significant predictor of good CKD knowledge, underscores the importance of kidney disease patient education provided by pharmacists. Congruent with our result, a similar study found higher knowledge scores among participants that reported seeing a CKD educator [21]. Furthermore, it has been reported that educational interventions prolong the time to dialysis initiation in patients near renal replacement [35]. Like other essential members of the multidisciplinary renal care team, asides from drug-related roles, a clinical pharmacist can help fill the knowledge gap of patients with CKD about the disease and lifestyle modifications to slow the progression of the disease. On the other hand, the likelihood of older participants having better knowledge than the younger ones may be due to their longer time with the disease and increased access to information about the disease and its management from health professionals.
The main strength of the study was the utilisation of two centres to control different hospital environment features. Other strengths were randomisation, blinding of participants about the investigators’ profession to avoid bias and a 12-month follow-up. The study did, however, have certain limitations. Patients that were included in the study may differ from those who did not participate in some important aspects, which may limit the generalisability of the study findings. Another weakness of the study was attrition bias or loss during follow-up. Although the tool used is valid and reliable, the data on CKD knowledge was self-reported.
Conclusion
Clinical pharmacists’ educational interventions led to a significant improvement in the CKD knowledge of patients with pre-dialysis CKD. This demonstrates that the pharmacist is a neglected but critical renal care provider in the study setting. Therefore, further studies to evaluate the impact of the interventions provided on healthcare-seeking behaviours, and self-management practices are warranted. As a result, there is a need for healthcare policies that include other healthcare professionals, such as pharmacists, in renal care in LMICs. This strategy has the capacity to improve the quality of care provided to patients with CKD. Finally, more studies are also required to investigate the long-term economical and clinical outcomes of this type of educational programme.
Acknowledgement
The authors are grateful to all the study participants for making themselves available for this study.
Conflict of Interest
This study has no conflict of interest. This research did not receive any specific grant from funding agencies in public, commercial or not-for-profit sectors.
Reference
- Okoro RN, Farate VT. Evaluation of potential drug–drug interactions among patients with chronic kidney disease in northeastern Nigeria. African Journal of Nephrology. 2019;22(1):77-81.
Doi: https://doi.org/10.21804/22-1-3577 - Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351(13):1296-305.
Doi: https://doi.org/10.1056/NEJMoa041031 - Levey AS, Schoolwerth AC, Burrows NR, et al. Comprehensive public health strategies for preventing the development, progression, and complications of CKD: Report of an expert panel convened by the Centers for Disease Control and Prevention. Am J Kid Dis. 2009;53(3):522-35. Doi: https://doi.org/10.1053/j.ajkd.2008.11.019
- Sever PS, Dahlof B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm (ASCOT-LLA): a multicenter randomised controlled trial. Lancet. 2003;361(9364):1149-58. Doi: https://doi.org/10.1016/S0140-6736(03)12948-0
- Lewis EJ, Hunsicker LG, Clarke WR, et al. Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med. 2001;345(12):851- 60. Doi: https://doi.org/10.1056/NEJMoa011303
- Jain D, Green JA. Health literacy in kidney disease: Review of the literature and implications for clinical practice. World Journal of Nephrology. 2016;5(2):147-51.
Doi: https://doi.org/10.5527/wjn.v5.i2.147 - Sakraida TJ, Robinson MV. Health Literacy Self-Management by Patients with Type 2 Diabetes and Stage 3 Chronic Kidney Disease. West J Nurs Res. 2009;31(5):627-47. Doi: https://doi.org/10.1177/0193945909334096
- Coresh J, Byrd-Holt D, Astor BC, et al. Chronic kidney disease awareness, prevalence, and trends among U.S. adults, 1999 to 2000. J Am Soc Nephrol. 2005;16(1):180-8. Doi: https://doi.org/10.1681/ASN.2004070539
- Finkelstein FO, Story K, Firanek C, et al. Perceived knowledge among patients cared for by nephrologists about chronic kidney disease and end-stage renal disease therapies. Kidney Int. 2008;74(9):1178-84. Doi: https://doi.org/10.1038/ki.2008.376
- [Schatell D, Ellstrom-Calder A, Alt PS, et al. Survey of CKD patients reveals significant GAPS in knowledge about kidney disease. Part 1. Nephrol News Issues. 2003;17(5):23-6.
- Schatell D, Ellstrom-Calder A, Alt PS, et al. Survey of CKD patients reveals significant gaps in knowledge about kidney disease. Part 2. Nephrol News Issues. 2003;17(6):17-9.
- Rantanen M, Kallio T, Johansson K, et al. Knowledge Expectations of Patients on Dialysis Treatment. Nephrol Nurs J. 2008;35(3):249-55.
- Costantini L, Beanlands H, McCay E, et al. The self-management experience of people with mild to moderate chronic kidney disease. Nephrol Nurs J. 2008;35(2):147-55.
- Lewis AL, Stabler KA, Welch JL. Perceived informational needs, problems, or concerns among patients with Stage 4 Chronic Kidney Disease. Nephrol Nurs J. 2010;37(2):143-8.
- Jennette CE, Vupputuri S, Hogan SL, et al. Community perspectives on kidney disease and health promotion from at-risk populations in rural North Carolina, USA. Rural Remote Health. 2010;10(2):1388. http://dx.doi.org/10.22605/rrh1388
- Devins GM, Mendelssohn DC, Barre PE, et al. Predialysis psychoeducational intervention extends survival in CKD: a 20-year follow-up. Am J Kidney Dis. 2005;46(6):1088-98. Doi: https://doi.org/10.1053/j.ajkd.2005.08.017
- Sealed Envelope Ltd. Power calculator for binary outcome superiority trial. [cited 2019 Nov 08]. Available from: https://www.sealedenvelope .com/power/binary-superiority/
- Sealed Envelope Ltd. Create a blocked randomisation list. [cited 2019 Nov 08]. Available from: https://www.sealedenvelope.com/simple- randomiser/v1/lists
- NIH (NIDDK). Kidney Disease Education Lesson Builder. 2014. https://www.niddk.nih.gov/health-information/communication-programms/nkdep/ Accessed August 01, 2018
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease. Am J Kidney Dis. 2002;39(2):S11-S12. Doi: https://doi.org/10.1016/S0272-6386(02)70084-X
- Wright J, Wallston KA, Elasy TA, et al. Development and results of a kidney disease knowledge survey given to patients with CKD. Am J Kidney Dis. 2011;57(3):387-95. Doi: https://doi.org/10.1053/j.ajkd.2010.09.018
- Levey AS, Coresh J, Greene T, et al. Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med. 2006;145(4):247-54. Doi: https://doi.org/10.7326/0003-4819-145-4-200608150-00004
- National Kidney Foundation (NKF). MDRD Study Equation. 2017. [cited 2019 July 27]. Available from: https://www.kidney.org/content/mdrd-study-equation
- Bloom BS. Taxonomy of educational objectives, handbook I: The cognitive domain. New York: David McKay Co Inc. 1956.
- Ulasi II, Ijoma CK. The enormity of chronic kidney disease in Nigeria: the situation in a teaching hospital in south-east Nigeria. J Trop Med. 2010. Doi: https://doi.org/10.1155/2010/501957
- Riegel B, Moser DK, Anker SD, et al. State of the science: Promoting self-care in persons with heart failure: A scientific statement from the American Heart Association. Circulation. 2009;120(2):1141-63. Doi: https://doi.org/10.1161/CIRCULATIONAHA.109.192628
- Steinsbekk A, Rygg L, Lisulo M, et al. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv Res, 2012;12:213. Doi: https://doi.org/10.1186/1472-6963-12-213
- Hurley J, Gerkin RD, Fahy B, et al. Meta-analysis of self-management education for patients with chronic obstructive pulmonary disease. Southwest Journal of Pulmonary, Critical Care and Sleep. 2012;4:194- 202 http://dx.doi.org/10.52494/KWQH7710
- Baby B, Antony CL, Wilson S, et al. Evaluation of the impact of pharmaceutical care on improving knowledge and medication adherence in CKD patients. Int J Pharm Pharm Sci. 2017;9(1):63-6. Doi: https://doi.org/10.22159/ijpps.2017v9i1.15053
- Khokhar A, Khan YH, Mallhi TH, et al. Effectiveness of pharmacist intervention model for chronic kidney disease patients; a prospective comparative study. Intl J Clin Pharm. 2020. Doi: https://doi.org/10.1007/s11096-020-00982-w
- Choi ES, Lee J. Effects of a Face-to-face Self-management Program on Knowledge, Self-care Practice and Kidney Function in Patients with Chronic Kidney Disease before the Renal Replacement Therapy. J Korean Acad Nurs. 2012;42(7):1070-8. Doi: https://doi.org/10.4040/jkan.2012.42.7.1070
- Kim AY, Kim SJ. The effect of education program on early hemodialysis patients’ knowledge, self-care practice and physiologic index. The Seoul Journal of Nursing, 2008;13(1):95-109.
- Ghimirey A, Sapkota B, Shrestha S, et al. Evaluation of pharmacist counseling in improving knowledge, attitude, and practice in chronic kidney disease patients. SAGE Open Medicine. 2013. Doi: https://doi.org/10.1177/2050312113516111
- Gray NA, Kapojos JK, Burke MT, et al. Patient kidney disease knowledge remains inadequate with standard nephrology outpatient care. Clinical Kidney Journal. 2016;9(1):113-8. Doi: https://doi.org/10.1093/ckj/sfv108
- Devins GM, Mendelssohn DC, Barre PE, Binik YM. Predialysis psychoeducational intervention and coping styles influence time to dialysis in chronic kidney disease. Am J Kidney Dis. 2003;42(4):693- 703. Doi: https://doi.org/10.1016/s0272-6386(03)00835-7
Please cite this article as:
Roland Nnaemeka Okoro, Ibrahim Ummate, John David Ohieku, Sani Ibn Yakubu and Maxwell Ogochukwu Adibe, Evaluation of the Impact of Clinical Pharmacists’ Educational Intervention on the Knowledge of Patients with Chronic Kidney Disease. Malaysian Journal of Pharmacy (MJP). 2022;2(8):16-26. https://mjpharm.org/evaluation-of-the-impact-of-clinical-pharmacists-educational-intervention-on-the-knowledge-of-patients-with-chronic-kidney-disease/