Abstract
This study aimed to assess the adequacy of EQ-5D-5L in defining health as perceived by Malaysians using a mixed methodology approach. Potential additional dimensions (i.e. bolt-on items) to supplement the current instrument were also explored. This study was carried out in two phases. In phase one, focus group discussions (N = 6-8 in each group) were employed to gauge the perception of Malaysians on the dimensions deemed important additions to the EQ-5D-5L instrument. Phase two involved further validation of bolt-ons to the EQ-5D-5L using a cross-sectional survey of 100 general public in Penang, Malaysia. A total of 11 bolt-ons were identified from phase 1. These bolt-ons were sleep, vitality, happiness, close relationships, stress, mental abilities, social support, religion, vision, hearing, and speaking. In phase 2, the bolt-ons of ‘vitality’ and ‘stress’ stood out with 70% (n=70) and 64% (n=64) participants reported facing most problems with, respectively. Both phases of study suggest that additional dimensions for the existing EQ-5D-5L instrument may be useful to better capture the HRQoL among Malaysians. Larger scale study is warranted to further validate the bolt-ons identified in this study.
Introduction
Health-related quality of life (HRQoL) instruments offer a way to measure patient-reported outcomes in addition to existing clinical indicators for a more wholesome assessment of a person’s well-being [1]. Currently, these instruments are widely applied in economic valuations, besides quantifying the effectiveness of medical treatments, and monitoring patients’ medical progress [2]. One of the most commonly used generic HRQoL measures is the EuroQol five-dimensional questionnaire (EQ-5D). The EQ-5D instrument comprises five dimensions, namely mobility, self-care, usual activities, pain/ discomfort and anxiety/depression [3]. The EQ visual analogue scale (EQ-VAS) usually accompanies the 5 earlier questions and measures general health on a thermometer-like scale from 0 (worst possible health imaginable) to 100 (best possible health imaginable) [4]. Designed with simplicity in mind, the original EQ-5D has three levels (known as EQ-5D-3L) of severity ranging from ‘no problem’ to ‘unable to’ perform a specific task. However, having suffered from ceiling effects [5][6], a newer version with five levels of severity (EQ-5D-5L) has been introduced since 2009 [7]. In tandem with the growth of health technology assessment in Malaysia, the application of the EQ-5D5L instrument has been increasingly utilised in the country [8]. Importantly, the concept and application of HRQoL, being subjective in nature, has shown to be influenced by both culture and socioeconomic status [9][10], and these differences may extend between the context of Malaysia and the European countries in which the instrument was originally developed. A recent study [11] conducted on the data of 51 countries of the World Values Survey indicated that self-reported health is indeed associated with cultural values that differ between countries. Therefore, the dimensions included in the EQ-5D-5L instrument, which was developed and catered to the European population, may not truly reflect how Asians choose to define health.
Having a HRQoL tool that fits the need of the local population would mean that the scope of dimensions chosen reflects the definition of health as a population. HRQoL tools that functions alternatively as preference-based measures, such as the EQ-5D-5L can be used to generate health utilities. These health utilities sum up the values of the dimensions to quantify the value of health. Consequently, patientreported outcome measures (PROM), including the EQ-5D-5L must quantify health with only a selected number of health dimensions before becoming too burdensome on respondents. The choice of HRQoL dimensions to include in an instrument has far reaching implications, especially when used in economic evaluations. Health utilities that fail to reflect the true health concerns of a population will not be effective as outcome variables in quantifying or comparing benefits of different treatment approaches. In the initial stages of development, the interpretation and perception of the five health dimensions of EQ-5D-5L instrument were tested qualitatively in focus groups in different European populations [12], signifying that the dimensions chosen are suitable for the European populations. To date, there is no qualitative study done to determine how Asian populations (including Malaysians), perceive the dimensions of the EQ-5D-5L instrument and whether the scope of HRQoL fits the need of the local population.
Therefore, assessing the perception of Malaysians about the use of EQ-5D-5L will be timely to guide the application of this instrument. Furthermore, exploring additional dimensions (commonly known as bolt-ons) [13] that can supplement the EQ-5D-5L instrument will be useful to better capture the HRQoL needs of the Malaysian population. This study aimed to assess the adequacy of the EQ-5D-5L in defining health as perceived by Malaysians using a mixed methodology approach. Specifically, a qualitative approach was applied to study the perception of Malaysians on the EQ-5D-5L and EQ-VAS in describing the HRQoL and to explore potential bolt-ons to complement the existing EQ-5D-5L instrument and subsequently, a quantitative approach was used to explore the suitability of the bolt-ons
Methods
This study was divided into two phases. Focus group discussions were held in the first phase with the aims to gauge the perception and understanding of Malaysian population on the original EQ-5D-5L instrument and subsequently, to explore additional dimension(s) (if any) to strengthen the instrument. In the second phase, the effects of bolt-ons (based on findings in phase 1) to the EQ-5D-5L descriptive instrument were further studied. Ethics approval has been granted by the Malaysia Medical Research & Ethics Committee (ID NMRR-13-1377-18574).
Study Population and Setting
In phase 1, focus groups comprised of 6 to 8 participants each, were conducted. The inclusion criteria for participant recruitment were Malaysians aged between 30 and 50 years who were able to converse in Malay or English. Participants were recruited via purposive sampling to ensure that the final cohort had a healthy mix of different gender, ethnicity and age, whilst adhering to the inclusion criteria and written consents were also obtained. The focus groups were held in Universiti Sains Malaysia, Penang. A semi-structured interview guide was used in the discussion and the number of focus groups conducted was determined by data saturation. Topics of discussion included understanding of the five dimensions in the EQ-5D-5L, factors influencing the EQ-VAS scores, and any other aspects perceived to affect their definition of health and HRQoL. Both sessions were conducted in a mix of the Malay and English languages to facilitate delivery of ideas where participants were informed that they could speak their preferred language and each session was audio recorded.
Phase 2 of the study was a cross-sectional survey that involved 100 conveniently sampled general public. Malaysians aged 18 years and above, and were able to speak or write in Malay or English were recruited. The questionnaire was self-completed by the respondents and assistance was provided when clarification was required. The questionnaire consisted of five parts, namely socio-demographic information, self-reported health using EQ-5D-5L descriptive instrument, bolt-ons structured in the same manner as the EQ-5D-5L descriptive instrument (identified from Phase 1) (APPENDIX 1), EQ visual analogue scale (EQ-VAS), and the ease of understanding of the EQ-5D-5L and bolt-ons using a 5-point Likert type scale (1= very easy to understand, 5= very difficult to understand) (as shown in Appendix). The questionnaire was available in both Malay and English languages.
Data Analysis
The focus group audio recordings were independently transcribed verbatim by two researchers and crosschecked for inconsistency. The finalized transcriptions were analysed for emergent themes using the framework approach, as described elsewhere [14]. Basically, the framework approach involves systematically summarizing the data of the transcript into a framework matrix to facilitate clear interpretation of underlying themes or concepts. All co-investigators were involved in discussing to reach a consensus on themes, codes, and representative quotes.
Descriptive analysis was applied in phase 2. The frequencies and percentages of all variables, together with mean and standard deviation of continuous variables were presented in table forms. Chi-square test was used to test the relationship between various categorical socio-demographic variables and the ease of understanding of each dimension, Fisher’s Exact Probability Test for 2 x 2 tables with frequencies less than 10, while Mann-Whitney test was applied for continuous variables. The ease of understanding responses of each dimension was grouped into two, those who answered “very easy” or “easy” and those who answered “moderate” or higher. Data were analysed using SPSS Statistics version 22 (IBM, Illinois) and p-value of < 0.05 was considered statistically significant.
Results
Phase 1: Focus Group Discussions
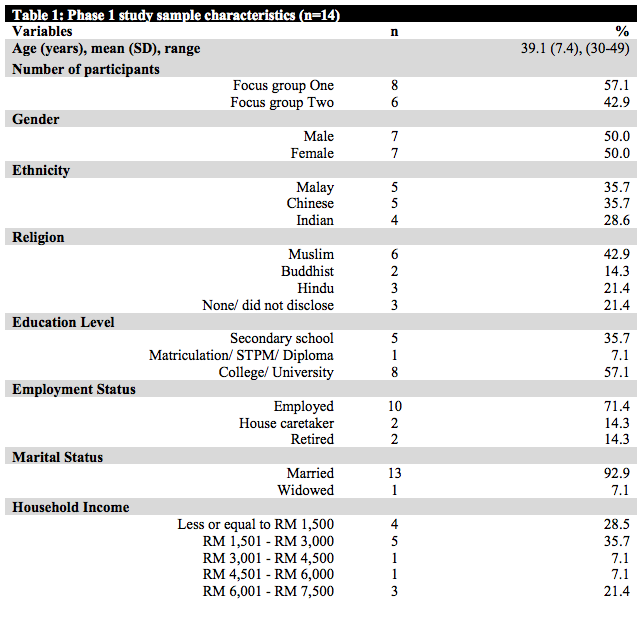
Data saturation was reached after two intensive discussion sessions. The recruited participants comprised a mix of the major races in the Malaysian population i.e. Malay, Chinese, and Indian (Table 1). Each focus group lasted for about one and a half hour. Opinions expressed in Malay were later translated to English and face validated by a native speaker investigator prior to data analysis. Three themes were identified in phase 1:
i) Understanding about EQ-5D-5L
Generally, the participants found all five dimensions in EQ-5D-5L were easy to comprehend. The mobility dimension was generally interpreted as only walking abilities as stated in the severity descriptions of the dimension in the instrument,
“Looking from the statements, it is already written here problems with walking, so I presume that mobility (dimension) refers to walking. So, I am answering the question based on the word ‘walking’ (abilities) and not the general word of mobility.”
(Female, 31, Chinese)
The self-care dimension was interpreted by most respondents as the ability to carry out one’s basic and daily activities,
“To me, the second dimension (self-care) describes the ability of a person to care for himself. That is what I understand. Whether a person is able to perform his daily activities independently or whether he needs assistance or not in terms of bathing, wearing clothes, cleaning…”
(Male, 33, Malay)
Participants perceived the usual activities dimension as their daily routines,
“Usual activities are things such as going to and coming back from work. Seems like that. Activities that we usually perform daily.”
(Male, 32, Malay)
Comparatively, more respondents were facing problems themselves in the dimension of pain/discomfort and anxiety/depression and therefore were explaining their own experiences in facing those health issues. The pain/ discomfort dimension was perceived to encompass either physical discomforts or pains,
“The (dimension) that is having pain, a slight pain. I just twisted my back because of hiking or something else. I’m not too sure. Yeah, so I have got some slight discomfort.”
(Male, 48, Chinese)
Nearly all participants associated anxiety/depression dimension as having the feeling of worry due to stressful life events,
“…my son just coming home from hospital (after a dengue infection). He is going to sit for an exam tomorrow. So, I am worried about his health. He is not fit yet. So I am just worried and then Deepavali is around the corner. So with all this, I am a housewife and I am also working, so the (whole thing) is stressful.”
(Female, 48, Indian)
ii) Factors influencing the score of EQ-VAS
One of the key factors affecting the rating of EQ-VAS was the existing environmental problem,
“I score 50 for today because of the haze and cough. As for the kids, they will also be having the cough causing their health to become worse.”
(Male, 33, Indian)
“I scored 70 because of the terrible haze last week. Everything is related to haze. For example, when I wanted to do some outdoor activities, like playing ball in the open air, the breathing is badly affected. It’s bad.”
(Male, 32, Malay)
Whilst some of the participants rated their EQ-VAS score based on measurable HRQoL factors such as obtaining sufficient sleep or having physical pains after vigorous sports, others chose to rate their health based on being able complete unfinished business or spend quality time with family,
“I rate my scale as 85 because we had Eid holidays and I was able to spend a lot of quality time with my child and wife.”
(Male, 32, Malay)
iii) The concept and dimensions of ‘health’
The participants were asked to define “health” and discuss about various aspects affecting their health. Interestingly, the majority of the participants emphasized on the importance of the mental and social aspects in defining good health,
“If you’re mentally not healthy, then you will easily commit suicide, and you will still not be in a complete health state. In terms of social, we need to interact with people. Only we interact with people then we share our problems, (receive) encouragement from peers. That definitely will help to build the more complete health state. So I think both elements (mental and social) are important.”
(Female, 33, Chinese)
Besides, there were others who stressed upon the spiritual aspect in affecting people’s health, “Okay, to me, an individual has to be healthy from the inside, spiritually. Viewing from a Muslim perspective, when we pray or read the Quran, so, the inner self will reflect our outer self. Being loyal to God will allow us to be healthier and calmer.”
(Male, 33, Malay)
‘Sleep’ was also commonly deemed as an important dimension to influence health, with participants sharing their experience of developing chronic diseases and nervous breakdowns as a result of lacking sleep,
“I put sleep as number one because if you don’t get enough sleep, the disease will just break in. Hypertension, heart attack… And all this start from the sleep, don’t have enough rest and even with a little bit of tension you cannot handle because the brain is too tired.”
(Female, 48, Indian)
The feeling of stress, especially due to the workload and uncompleted tasks was prevalent among some participants. The stress often affects health in a negative way,
“Feeling unhealthy because of stressing up with work…Or anything else that you have unfinished business. Then you feel unhappy with the thing until you complete it or at least attempt to complete it.”
(Male, 36, Indian)
Social support was perceived by a number of participants as another influential factor affecting health as it helps people overcome the stresses of daily living,
“… and social support has to be there to support everybody to take through their daily living so if you can’t do daily living properly, then you are going to get stressed and back to the same circle certainly.”
(Male, 36, Indian)
Factors that have been deemed important to influence HRQoL by two or more participants were then considered as bolt-ons. In total, 11 bolt-ons were identified include sleeping, social support, vitality, happiness, close relationships, stress, mental abilities, religion, vision, hearing, and speaking. These were further tested in phase 2.
Phase 2: Bolt-On Survey
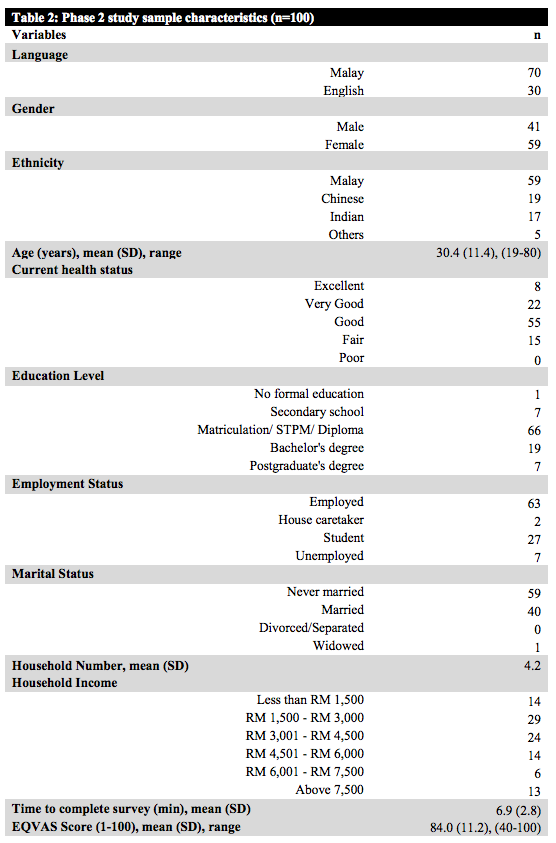
The demographics of the 100 participants are shown in Table 2. 95% of the survey participants claimed that their comprehension level of the EQ-5D-5L descriptive instrument with bolt-ons ranged between 1 (very easy to understand) to 2 (easy) of the 5-point Likert scale, and no one reported a comprehension level of higher than 3 (moderate).
In general, responses of moderate on the bolt-on descriptive instrument tended to come from those whose highest educational qualification was pre-university level (matriculation/STPM/diploma), male gender. No obvious trend was observed for age, marital status, income, and household number. However, no statistical significance was reached on the test of associations on all the bolt-on dimensions. In the original EQ-5D-5L dimensions, similar trends were observed, and none of the sociodemographic variables were statistically associated to the responses, except gender where only males reported moderate ease of comprehension.
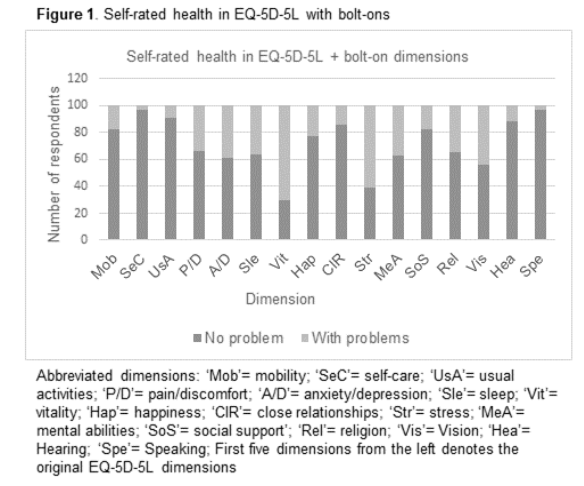
In assessing their self-reported on the pain/discomfort dimension health problem on the EQ-5D-5L descriptive instrument, the majority of participants reported facing no problems in the five original health dimensions (Figure 1). Of the 5 dimensions, the highest self-reported problems (ranging from slight problems to extreme problems) were associated with anxiety/depression (39%) and pain/discomfort (34%). Comparatively, of the bolt-ons, two particular dimensions, i.e. vitality (70%) and stress (61%) denoted most significant amount of self-reported problems among the 100 participants.
Discussion
Overall, all participants showed good understanding of the individual 5 dimensions in EQ-5D-5L in both phase 1 and 2. The simple way the original EQ-5D-5L dimensions were worded was used as a basis to which the bolt-ons were constructed. This factor could have contributed to at least 95% of the respondents stating the EQ-5D-5L descriptive instrument with bolt-ons questions were either very easy or easy to understand and subsequently ease of understanding of the bolt-ons was also not associated with any socioeconomic factors. Comprehension level for the bolt-ons was not affected by age, gender, education level, employment status, marital status, income and household number.
This is in line with the intentions of the developers of the EQ-5D-5L instrument for easy administration of this HRQoL assessment tool. Past qualitative studies conducted in the early stages of development of the EQ-5D instrument showed that even among health researchers, the meaning of terms used to describe dimensions may be interpreted variably [12]. This led to the EuroQol Group initiating an outline to define key concepts of the instrument with primary uses in translating the EQ-5D into different languages. Having proper understanding of the dimensions is important to ensure comparability and validity among studies conducted in different setting and countries.
The EQ-VAS, being part of the measure of general health in EQ-5D-5L, captured a wider range of issues that might influence individual perception of own health, from the usual physical illness to subjective matters such as spending enough time with one’s loved ones. Observing the wide spectrum of reasons for the EQ-VAS responses of participants, the visual analogue scale may be better used as a complementary HRQoL tool, rather than a stand-alone tool considering that perception and rating of ‘health’ may vary significantly among individuals. However, the existence of a global health question such as the EQ-VAS allow perceptions of health that may not be collectively be shared by the majority of the population, be captured by a number ranging from zero to 100.
The concept of health or HRQoL is generally accepted to encompass physical, mental, and social wellbeing. Focus group discussions revealed that personal definitions of health may vary slightly but there are recurring concepts of health that are shared by many. Of the 11 bolt-on suggested, 5 can be classified as physical abilities (speaking, hearing, vision, vitality, sleep), 3 under mental concepts (mental abilities, happiness, stress), and the remaining 3 under social concepts (close relationships, social support, religion).
In structuring the concepts for the bolt-ons, similar wordings were used to describe the Likert scale with no problems being the first option and extreme problems being the last option. Only the religion bolton, being a more abstract concept, was worded differently with emphasis of religious belief to one’s approach in life (from entire dependence on religion to none at all on the Likert scale). The dimension of vitality, of which respondents collectively reported having most problems with (70% in this study), showed similar trend as in another large-scale EQ-5D-3L bolt-on study in Switzerland. The dimension was defined as ‘energy/fatigue [15] in that study, and the description was quite similar to our description for vitality, despite a different term was used. Although the Swiss study involved randomly selected general population aged 20 and above, no information on how representative the sample were. Therefore, it cannot be said for certain that vitality is a culturally prevailing dimension for the Swiss population, only that adding this dimension to the original EQ-5D dimensions help to explain the variance (R2 ) when regressed onto the EQ-VAS.
Stress is another dimension in this study with a higher percentage of respondents reporting having problem with. Surprisingly, stress has never been suggested in any previous EQ-5D-3L bolt-on studies. This could be because most of the past studies were conducted to address instrument limitations in condition-specific cases. The dimension of stress may be perceived as too general to test for in condition specific studies. Also, the factor of culture may come into play. The dimension was included in the phase 2 of our study as it was frequently highlighted in the focus group discussions (phase 1) as an important factor associated with feeling unhealthy. This feeling of un-healthiness was usually triggered by a variety of personal or work-related stressors and indeed, stress is often linked to poorer well-being and increased health issues [16].
Past bolt-on studies have been conducted in Southern Yorkshire, UK or the Netherlands where five additional dimensions including tiredness, vision, hearing [17], cognition [18] and sleep [19] have been tested. The former four dimensions were shown to significantly impact health state values in their utility index while only the sleep dimension was deemed less significant. Contrarily, a recent bolt-on study on the EQ-5D-3L instrument in Cape Town, South Africa [20] added sleep and concentration as bolt-ons as means to explain the variance of health in community based-populations. The bolt-ons did increase the explanatory power of the original instrument when the EQ visual analogue scale (EQ-VAS) was used as the dependent variable. Additionally, a vision bolt-on study conducted in Singapore [21] demonstrated that adding vision bolt-on to the existing EQ-5D-3L instrument better discriminated those with different levels of vision problems. The study suggested the index score of EQ-5D-3L with vision bolt-on was significantly more sensitive than the standard EQ-5D-3L index score in detecting changes of people with varying levels of visual impairment. However, it is to be noted that the study focused on discriminating different levels of visual impairment using the bolt-on index, and not deriving new boltons based on differences in cultural values.
Depending on the populations and methods of testing used, the results of bolt-on studies generally vary in various countries with different cultures. A standardisation of methodology in bolt-on studies carried out in different populations may assist in revealing the true usefulness of particular bolt-on(s). There are a few limitations in this study. Our study was conducted in the state of Penang, thus may not be generalizable to the whole of Malaysia. Also, phase 2 of the study only captured the self-reported health problems as reflected by the EQ-5D-5L descriptive instrument together with bolt-ons. No preference-based valuation method was employed to quantify the explicit value of additional dimensions to better scope the need of such bolt-ons. Being an exploratory study, the sample size employed was small and the methodology was simple. Possible bias in the study might arise from the convenience sampling design of phase 2. The over-sampling of those who have employment may have skewed the results to favour vitality and stress as the two dimensions with highest reported problems. However, to the best of our knowledge, our study was the first in Malaysia and Southeast Asia to explore potential bolt-ons based on local culture and social-economic status. Observing that bolt-ons vitality and stress have more than half of the respondents reporting problem in them, these could be two additional dimensions worthy of more emphasis in future HRQoL studies. Therefore, it is hoped that the preliminary results of this study will provide insights into guiding the selection of bolt-ons for larger scale validation studies in the near future.
Conclusion
In our study, the HRQoL concept was seen to encompass a wider scope than currently covered by the EQ-5D-5L instrument, with the vitality and stress having most potential for bolt-ons in future valuation studies. This study suggested that the prospect of adding bolt-ons to complement the EQ-5D-5L instrument would better suit the HRQoL needs of the Malaysian population.
Acknowledgements
We would like to extend our gratification to the following undergraduate pharmacy students for their assistance in the study- Chiew YK, Teoh AXY, Jayakumar T, Tan RS, Wong XM, Koh Y, Mohd Nazdmi MAN, Thum CS, Kamarul Zaman MA, and Mohd Ali NA. This study was funded under the Research University Grant by Universiti Sains Malaysia (1001/PFARMASI/811287).
References
- Fayers PM, Machin D. Quality of life: Assessment, Analysis and Interpretation. England, UK: John Wiley & Sons, Ltd.; 2000.
- Feng Y, Devlin N, Herdman M. Assessing the health of the general population in England: how do the three- and five-level versions of EQ-5D compare? Health and Quality of Life Outcomes. 2015;13(1):1-16. doi: 10.1186/s12955-015-0356-8.
- Brooks R. Introduction. In: Brooks R, Rabin R, De Charro F, editors. The measurement and valuation of health status using EQ-5D: a European perspective: evidence from the EuroQol BIO MED research programme. The Netherlands: Kluwer Academic Publishers; 2003. p. 1-6.
- Krabbe PF, Weijnen T. Guidelines for analysing and reporting EQ-5D outcomes. In: Brooks R, Rabin R, De Charro F, editors. The measurement and valuation of health status using EQ-5D: a European perspective: evidence from the EuroQol BIO MED research programme. The Netherlands: Kluwer Academic Publishers; 2003. p. 1-6.
- Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727-36. Epub 2011/04/12. doi: 10.1007/s11136-011-9903-x [doi]. PubMed PMID: 21479777; PubMed Central PMCID: PMC3220807.
- Lloyd A, Quadri N, editors. Testing alternative labels for a UK English five level version of EQ5D. 25th Scientific Plenary Meeting of the EuroQol Group; 2008; Baveno Lake Maggiore, Italy: EuroQol Group.
- Devlin NJ, Brooks R. EQ-5D and the EuroQol Group: Past, Present and Future. Applied Health
Economics and Health Policy. 2017;15(2):127-37. doi: 10.1007/s40258-017-0310-5. - Shafie AA. EuroQol 5-Dimension measures in Malaysia. In: Michalos AC, editor. Encyclopedia of Quality of Life and Well-Being Research: Springer; 2014. p. 2041-4.
- Backett KC, Davison C. Lifecourse and lifestyle: The social and cultural location of health
behaviours. Soc Sci Med. 1995;40(5):629-38. doi: http://dx.doi.org/10.1016/0277-9536(95)80007- 7. - Collinge A, Rudell K, Bhui K. Quality of life assessment in non-Western cultures. Int Rev Psychiatry. 2002;14(3):212-8.
- Roudijk B, Donders R, Stalmeier P. Cultural values: can they explain self-reported health? Qual Life Res. 2017;26(6):1531-9. Epub 2017/02/12. doi: 10.1007/s11136-017-1512-x. PubMed PMID: 28185039; PubMed Central PMCID: PMCPMC5420378.
- Fox-Rushby J, Selai C. What concepts does the EQ-5D measure? intentions and interpretations. In: Brooks R, Rabin R, De Charro F, editors. The measurement and valuation of health status using EQ-5D: a European perspective: evidence from the EuroQol BIO MED research programme. The Netherlands: Kluwer Academic Publishers; 2003. p. 143-66.
- Longworth L, Yang Y, Young T, Mulhern B, Hernandez Alava M, Mukuria C, et al. Use of generic
and condition-specific measures of health-related quality of life in NICE decision-making: a systematic review, statistical modelling and survey. Health Technol Assess. 2014;18(9). doi: 10.3310/hta18090. - Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi: 10.1186/1471-2288-13-117.
- Perneger TV, Courvoisier DS. Exploration of health dimensions to be included in multi-attribute health-utility assessment. Int J Qual Health Care. 2011;23(1):52-9. Epub 2010/11/19. doi: 10.1093/intqhc/mzq068. PubMed PMID: 21084324.
- Schneiderman N, Ironson G, Siegel SD. STRESS AND HEALTH: Psychological, Behavioral, and
Biological Determinants. Annu Rev Clin Psychol. 2005;1:607-28. doi: 10.1146/annurev.clinpsy.1.102803.144141. PubMed PMID: PMC2568977. - Yang Y, Rowen D, Brazier J, Tsuchiya A, Young T, Longworth L. An exploratory study to test the impact on three “bolt-on” items to the EQ-5D. Value Health. 2015;18(1):52-60. doi: 10.1016/j.jval.2014.09.004. PubMed PMID: 25595234.
- Krabbe PF, Stouthard ME, Essink-Bot ML, Bonsel GJ. The effect of adding a cognitive dimension to the EuroQol multiattribute health-status classification system. J Clin Epidemiol. 1999;52(4):293-301 .PubMed PMID: 10235169.
- Yang Y, Brazier J, Tsuchiya A. Effect of adding a sleep dimension to the EQ-5D descriptive system: A “bolt-on” experiment. Med Decis Making. 2014;34(1):42-53. doi: 10.1177/0272989X13480428. PubMed PMID: edselc.2-52.0-84890605215.
- Jelsma J, Maart S. Should additional domains be added to the EQ-5D health-related quality of life instrument for community-based studies? An analytical descriptive study. Population Health Metrics. 2015;13(1):13. PubMed PMID: doi:10.1186/s12963-015-0046-0.
- Luo N, Wang X, Ang M, Finkelstein EA, Aung T, Wong T-Y, et al. A Vision “Bolt-On” Item Could
Increase the Discriminatory Power of the EQ-5D Index Score. Value Health. 2015;18(8):1037-42. doi: http://dx.doi.org/10.1016/j.jval.2015.08.002.
Please cite this article as:
Thakumar AV, Shafie AA and Lim CJ, Exploration of EQ-5D-5L Bolt-On Items among Malaysian Population. Malaysian Journal of Pharmacy (MJP). 2017;1(3):8-17. https://mjpharm.org/exploration-of-eq-5d-5l-bolt-on-items-among-malaysian-population/