Abstract
Benign Prostatic Hyperplasia (BPH) is a hyperplasia process where there are an increased number of cells from the transition zone of the gland. The goals of the study were: (1) to compare the effectiveness of finasteride 5mg (Proscar) versus alfuzosin 10mg (Xatral XL) for the treatment of BPH; (2) to compare the treatment costs of both drug; (3) to compare the side-effect profile of both drug. All patients who have been diagnosed with BPH and have been receiving the treatment in SOPD Hospital Tuanku Ja’afar were reviewed. The inclusion criteria were: (1) male more than 45 year old; (2) patients who are not suffering from recurrent or rebound BPH. Subjects were evaluated using the International Prostate Symptom Score (IPSS) questionnaire The score and side effects occurrence were analysis by SPSS. Only 66 men were analyzed in the study as 6 men (8.3%) were excluded. 36 of them (55%) are taking Finasteride 5mg once daily whereas the other 30 men (45%) are taking the extended released form of Alfuzosin 10mg once daily. The distribution of subject’s age is even. Subjects with Finasteride 5mg have higher score (mean = 22.18) than Alfuzosin 10mg (mean = 18.87) (p<0.05). However, the total side effect score of both drug showed no significant different (p>0.05). Finasteride group (mean = 0.52 case) has experienced a slightly more side effect than the Alfuzosin group (mean = 0.50 case). This study concluded that both Alfuzosin and Finasteride provide symptomatic relief to BPH patients. Alfuzosin with its faster onset of action could be very useful for patients who were diagnosed with BPH and carry moderate IPSS scores.
Introduction
Benign Prostatic Hyperplasia (BPH) is a hyperplasia process where there are an increased number of cells from the transition zone of the prostate gland. The prevalence of this condition increases with age and requires the presence of testicular androgens. About half of men’s population will develop BPH by the average of 50 years old, due to the complex stromal-epithelial interactions[1]. The disease can be progressive, showing symptoms which can be classified into two categories: irritative (frequency, nocturia, burning, urgency or urge incontinence) and obstructive (hesitancy, weak stream, dribbling, incomplete voiding or retention). Besides these bothersome lower urinary tract symptoms (LUTS), there could also be associated anatomic enlargement of the prostate leading to the compression of the urethra, resulting in compromised urinary flow and bladder outlet obstruction (BOD).
BPH symptoms manifested could interfere with patient’s daily living activities, causing significant impairment in the quality of life and in some cases compromised sexual functioning. Serious cases could also subsequently lead to secondary changes of the bladder anatomy and function, urinary tract infections, formation of bladder stones, and eventually causing the deterioration
of the upper urinary tract accompanied with renal failure.
Patients manifesting with different symptoms should be treated using different approaches. Most patients are first assessed by a quantitative symptom score, such as the International Prostate Symptom Score (IPSS) which was further applied in the present study. According to a study[2], an estimated 35 percent of elderly males need either surgical or medical intervention or both for BPH in their lifetime. However, surgical intervention was rather radical from most of the patient’ perspective and many of them were reluctant to undergo surgery and prefer a less invasive treatment. Patients are aware of the availability of effective pharmacotherapy and also have the awareness of the complications of surgery which can include significant morbidity such as irreversible incontinence and loss of sexual function. It is therefore not astounding that besides surgery and watchful waiting, medical management is generally the first recommendation for patients showing bothersome symptoms, although many do make it better without any intervention.
When treating BPH, drug therapy could always be an option to control symptoms and delay the need for surgical intervention. To decide the most appropriate medication to treat moderate to severe BPH, it is often crucial that the choice of drug depends on the actual or patient- perceived effectiveness of therapy, onset of action, adverse effects, dosing regimen, potential drug-drug interaction and cost. The goals of drug therapy are to provide symptomatic relief and to prevent any further complications. Drug therapy for BPH normally begins with a single therapeutic agent, usually an alpha-adrenergic antagonist. BPH medication treatment is always indicated for long period. Therefore, patient should always be advised that symptoms improvement could be observed only when treatment is continued and good adherence is observed.
Drug therapy for BPH can be classified into 2 different categories: agents that act directly on the prostatic smooth muscles and those that interfere with the stimulatory effects of testosterone on prostate enlargement. Of the agents, α1 adrenergic antagonists such as alfuzosin, doxazosin, terazosin relax prostatic smooth muscles, whereas 5-α reductase inhibitors such as finastride, selectively inhibit the conversion of testosterone to dihydrotestosterone. Both these agents are accepted for treatment of BPH. However, the difference in their mechanisms of action has rendered these agents in treating different clinical symptoms. Finasteride was found to work best with patients who have a significant
prostate enlargement of more than 40g in size. On the other hand, α1adrenergic antagonists are more effective in treating patients who manifest with BPH symptoms caused by excessive adrenergic tone in the prostatic stroma. Therefore, these antagonists are often commonly being considered to be an appropriate treatment for all patients regardless of prostate size.
FDA has currently approved four α adrenergic antagonists (doxazosin, terazosin, tamsulosin and alfuzosin) for lower urinary tract symptoms associated with BPH. These agents however showed equal benefits and all provide modest symptoms relief. The first generation of α blockers such as doxazosin, terazosin and prazosin are associated with significant vasodilatory actions. These α blockers are always associated with certain degrees of vasodilatory side-effects such as dizziness and postural hypotension and subsequently cause poor compliance to treatment.
Newer generations of α blockers, namely alfuzosin and tamsulosin, bind more prominently to the lower urinary tract tissues compared to vascular tissues. Reflecting this differential pattern of tissue binding, these agents have been found to be associated with a lower risk of significant vascular side-effects compared with the non-uroselective α inhibitors, despite having a significant effect in reducing BPH symptoms[3]. However, literature has revealed that tamsulosin appears to have a lower probability of causing postural hypotension, but higher chances of ejaculatory dysfunction than other α blockers.
The extended release (ER) form of alfuzosin (10mg once a day) has been used and approved by the United States Food and Drug Administration in 2003 for treating signs and symptoms of BPH based on clinical improvements of the irritative and obstructive urinary symptoms of the disease. A study mentioned in the literature3 had discussed a meta-analysis of 3 clinical trials studying the vasodilatory effects of the ER alfuzosin compared to placebo. In these studies, results had shown that the effects were similar to placebo and no significant changes in blood pressure were observed.
On the other hand, finasteride, a selective 5-α reductase inhibitor, acts through a different mechanism compared to α-blockers. It decreases the conversion of testosterone to dihydrotestosterone, a hormone primarily found in the prostate gland, testes, hair follicles and adrenal glands. Dihydrotestosterone is the primary contributing factor in the development or exacerbation of BPH and prostate cancer. Therefore, finasteride, by selectively inhibiting type II 5-α reductase, could progressively delay the development of BPH. Many studies have shown
that finasteride, when compared to placebo, has effectively reduced the volume of the prostate and enlarged prostate glands in men [4][5].
Methodology
We conducted a study to compare two BPH drugs with different mechanisms of action. The aims of the study were: (1) to compare the effectiveness of finasteride 5mg (Proscar) versus alfuzosin 10mg (Xatral XL) for the treatment of BPH; (2) to compare the treatment costs of both drug; (3) to compare the side-effect profile of both drug Subjects were patients who have been diagnosed with BPH and have been receiving the treatment in SOPD Hospital Tuanku Ja’afar. The inclusion criteria were: (1) male more than 45 year old; (2) patients who are not suffering from recurrent or rebound BPH. On the other hand, the exclusion criteria include: (1) patient who has multi-disease prior to the study; (2) patient who has undergone surgical intervention prior to the study; (3) patient who was taking any other traditional or complementary medicines.
Subjects were evaluated using the International Prostate Symptom Score (IPSS) questionnaire (Appendix I). This instrument evaluates the lower urinary tract symptoms for the past one month. Subjects were asked seven questions associated with the following symptoms: (1) incomplete emptying of bladder during urination; (2) frequency of urine in less than 2 hours; (3) intermittency that stopped and started again when urinated; (4) urgency (difficulty to postpone urination); (5) weak stream; (6) straining which push to begin urination; and (7) nocturia (the number of times the subject has to get up from bed to urinate at night). The rating ranged from 0 to 5 which represent the frequency of the above symptoms in the past one month. The total score of IPSS is calculated by sum up the individual scores. Based on the total score of IPSS, 0-7 means mildly symptoms; 8-19 means moderately symptoms and 20-35 means severely symptomatic.
Subjects were also asked about side- effects of the drugs based on the established side-effects profiles of the drugs. This was to help the researcher to evaluate the patient’s acceptance of the drug therapy. There was a total score of 10 for this question.
The data were analyzed using SPSS. The two treatment groups were compared using Student’s t-test. P- value less than 0.05 was considered statistically significant.
Results
A total of 72 men diagnosed with BPH were involved in the study. However, only 66 men were included in the analysis. Of the 72 patients, three were taking the combination treatment of finasteride 5mg and alfuzosin 10mg, 2 other patients had just started the treatment for less than 1 week, whereas 1 patient was known to have underlying disease (stroke). Therefore, 8.3% of the total patients were excluded from this study as they did not meet the inclusion criteria.
36 of the subjects (55%) received finasteride 5mg once daily, whereas the rest took the ER alfuzosin 10mg once daily. The distribution of patients included was fairly equal to help minimize any bias in patient selections. This is the true distribution of patients encountered by our hospital out-patient department as the stock movements of our integrated store were found to be collaborated with our patient numbers.
Table 1 column 2 presents the distribution of the subjects by age group. Twenty men (30%) were from 50 to 59 years, 18 men (27%) were from 60-69 years, and 22 men (34%) were from 70-79 years. Only a small proportion of the study population (9%) was more than 80 years old.
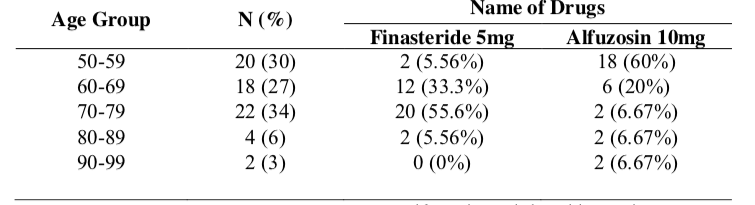
Table 1 Columns 2 and 3 shows the distribution of patients who received two different therapies for BPH, by age categories. In the finasteride group, about 33% of the patients were in the range of 60-69 years old, and more than half of the patients were aged 70-79 years. Conversely, in the alfuzosin group, the majority of the patients (80%) were between 50-69 years old. This shows the trend of drug prescribing in our hospital, where the younger patients were most probably prescribed with alfuzosin and the older patients were treated with finasteride.
Subjects who received finasteride 5mg had a significantly higher IPSS than those who received alfuzosin 10mg (mean IPSS of 22.18±8.06 vs.18.87±7.34, respectively; p=0.001). This indicates that patients who were treated with finasteride were severely symptomatic whereas those who received alfuzosin were moderately symptomatic (Table 2).

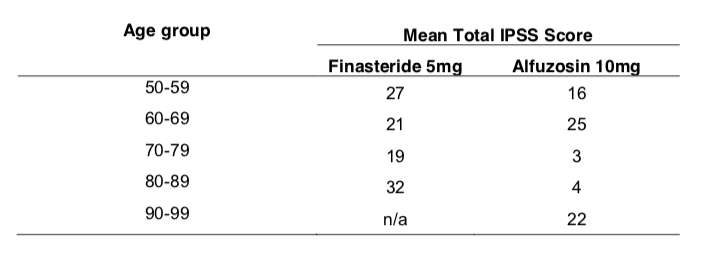
This study compared the mean IPSS of different age groups in the two treatment arms. Student’s t-test shows that there was no significant difference in IPSS between the two treatment arms across all age groups. Most of the groups obtained a mean IPSS of 20 and above, which indicates severely symptomatic patients (refer to Table 3).
The distribution of mean score based on duration of treatment of both drug is shown in the Table 4. The mean score of finasteride 5mg for less than half a year was 25; half a year to one year was 11; one year to 1.5 years was 30; and more than 1.5 years was 20. On the other hand, the mean score of alfuzosin 10mg for less than half a year was 20; half a year to one year was 21; one year to 1.5 years was 7; and more than 1.5 years was 10.

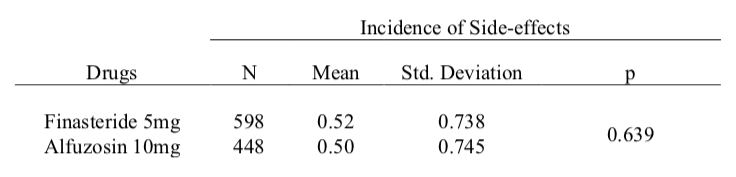
Table 5 shows no significant difference in the total side-effects scores between the two intervention groups (p=0.693). Overall, the finasteride group had experienced a slightly higher incidence of side- effects than the alfuzosin group (mean = 0.52 cases vs. 0.50 cases, respectively)
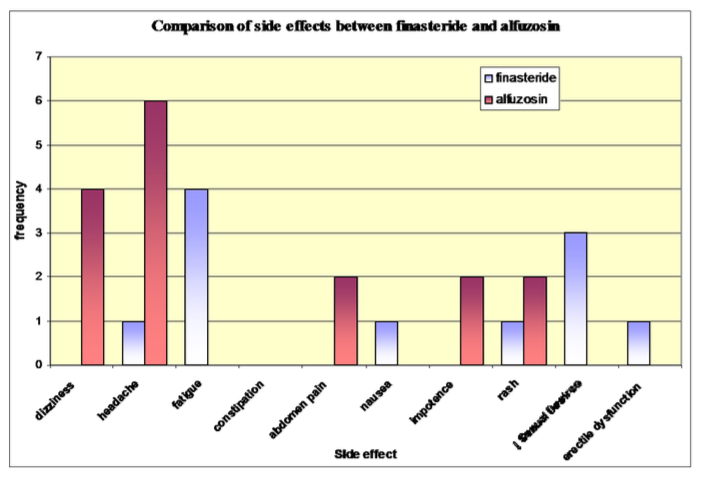
Figure 1 presents the frequencies of individual side-effects among the treatment groups. about 16.7% subjects on finasteride complained of fatigue and decreased sexual desires 5.6% experienced problems related to erectile dysfunction. Headache and dizziness contributed to 33.3%of side effects experienced by Alfuzosin arm.
In comparison of treatment costs between the two treatments, finasteride 5mg tablet (Proscar) was RM 123.00 per pack of 30’s while alfuzosin 10mg tablet (Xatral XL) was RM 41.31 per pack of 30’s. Treatment of BPH is often life long and effect will only be seen when the treatment is continued. Therefore, to consider a one-month treatment, alfuzosin can reduce cost by RM81.969 per month, contributing to RM980.28 every year.
Discussion
The most important finding of this study is that patients taking ER alfuzosin 10mg had a significantly lower International Prostate Symptom Score (IPSS) when compared to patients taking finasteride 5mg. BPH and its consequent bothersome lower urinary tract symptoms can severely affect quality of life in older men. On the basis of this study, we could deduce from the mean IPSS that alfuzosin provided a better improvement in the quality of life of these patients.
The study did not collect patients’ baseline values of the IPSS, therefore it is impossible for us to compare the effect before and after treatment. However, the finding showed that patients with higher IPSS scores (more severe) were normally prescribed finasteride 5mg. This observation could be seen as rational, since BPH is a progressive illness and significant prostate enlargement of more than 40g is normally a manifestation of the later stages of BPH. Progressive growth of the prostate would eventually overcome the reduction in prostatic urethral obstruction achieved by the relaxation of prostatic smooth muscle tone caused by alpha blockers even in patients on therapy[5].
One study which compared finastride with placebo showed symptomatic improvements in men with prostatic enlargement and moderate to severe symptoms[4]. Therefore, it would be logical to prescribe finasteride to patients who do not respond well with to alfuzosin and to minimize the need of surgical intervention as it is always an attribution to severe enlargement of prostate size. Patients treated with finasteride can eventually have a four-year risk reduction for surgical intervention and acute urinary retention[4]. The benefit of finasteride is slow, which can only be observed conservatively at about 4 months after initiation of therapy. Conversely, the effects of alfuzosin can be seen within first few days of treatment. The promptness of action of alfuzosin provides benefits of quick evaluation without delay and minimizes the costly long-term treatment where patients can only be re-evaluated after few months of inappropriate treatment.
The overall side effects between alfuzosin and finasteride shows no significant difference, with p>0.05. Patients from both arms shows different side-effects profiles, about 16.7% of patients treated with finastride had experienced fatigue and decreased sexual desires. 5.6% of them had encountered problems related to erectile dysfunction. These side-effects were mostly observed in patients receiving finastride for less than 1 year. On the other hand the most prominent side-effects experienced by patients taking alfuzosin were dizziness and headache. However, alfuzosin is generally reported to have only little effect on blood pressure when compared to other α blockers. Meta analyses of placebo and randomized controlled trials have demonstrated an extra 5%-20% of dizziness incidences reported by normotensive patients who underwent treatment with terazosin or doxazosin. However, with alfuzosin, the event of dizziness reported was approximately 5%6. In addition, one randomized controlled study found that the occurrence of postural hypotension with alfuzosin was at placebo level (estimated at 1%)7. This phenomenon is seen as alfuzosin is more selective to prostatic smooth muscle than vascular smooth muscles.
Another study estimated that about 30-50% of BPH patients would develop essential hypertension8. Patients who are originally on α- blocker as anti-hypertensive medications are more likely to experience cardiovascular adverse effects. Therefore, the second generation α-blockers such as alfuzosin are more suitable to this group of patients as they are more selective and could minimize the occurrence of cardiovascular side effects.
Conclusion
From the study, it is clear that both alfuzosin and finasteride provide symptomatic relief to BPH patients. However, the differences in mechanisms of actions of the two drugs made them useful to patients with different underlying problems. Alfuzosin with its faster onset of action could be very useful for patients who are diagnosed with BPH and carry moderate IPSS scores. Further studies need to be conducted in order to obtain a clearer picture of the efficacy and tolerability of both drugs.
Reference
- E. Darracott Vaughan, Jr., M. D. Medical Management of benign Prostatic Hyperplasia-Are two Drugs Better Than One N Eng J Med. 2003 Dec 18; Volume 349:2449-2451
- Oesterling JE. Benign prostatic hyperplasia: a review of its histogenesis and natural history. Prostate Suppl 1996;6:67-73
- Kevin T. McVary. Alfuzoxin for Symptomatic Benign Protatic hyperplasia: Long- Term Experience. Available online 12 December 2005
- John D. McConnell et al. The Effect of Finasteride on the Risk of Acute Urinary Retention and the Need for Surgical Treatment among Men with Benign Prostatic Hyperplasia. N Eng J Med. 1998 Feb 26;338(9):612-3
- John D. McConnell et al. The Long Term Effect of Doxazosin, Finasteride and Combination Therapy on the Clinical Progression of benign Prostatic Hyperplasia. The New England Journal of Medicine 2003 Dec 18;349(25):2387-98
- McKiernan JM, Lowe FC. Side effects of terazosin in the treatment of symptomatic benign prostatic hyperplasia. South Med J. 1997;90:509– 513.
- Christopher R. Chapple. A Comparison of Varying α-Blokers and Other Pharmacotherapy options for Lower Urinary Tract Symptoms. RevUrol. 2005; 7(Suppl 4):S22-S30
- Alfuzosin Hydrochloride for the Treatment of Benign Prostatic from American Journal of Health-System Pharmacy. Available online: www.medscape,com/viewarticle/458899_13
- A. Tejani et al; Clinical practice: Benign Prostatic Hypertrohpy. Available online : www.cfpc.ca/cfp/2006/Sep/vol52-sep-clinical-therapeutics.asp
Please cite this article as:
Lee Sau Yong, Tan Meng Wah and Wan Noor Hayati, The Study of Alfuzosin and Finasteride in the Treatment of Benign Prostatic Hyperplasia. Malaysian Journal of Pharmacy (MJP). 2008;6(1):234-245. https://mjpharm.org/the-study-of-alfuzosin-and-finasteride-in-the-treatment-of-benign-prostatic-hyperplasia/