ABSTRACT
Introduction: Conventional drug research and development encompasses multiple phases for identifying novel pharmaceuticals and securing marketing authorization. Consequently, repurposing or repositioning previously approved drugs to treat both common and rare diseases is becoming an increasingly appealing proposition. This approach involves the use of de-risked compounds, potentially lower overall development costs, and shorter development timelines. This review outlines drugs that have already been repurposed for treating various diseases, their mechanisms of action, and the current advantages, considerations, and challenges associated with drug repurposing. Methods: A literature search was conducted in Scopus, PubMed, Web of Science, and Google Scholar to screen for articles published from 2015 to 2025 that report the repurposing of drugs for diseases beyond their approved use. Approximately sixty studies were identified and discussed in this review, including repurposing of previously approved drugs for different neurological disorders, cancer, respiratory disorders, cardiovascular, and gastrointestinal (GIT) diseases. Results and Conclusion: The studies reviewed highlight the potential of drug repurposing as a cost-effective strategy for identifying new therapeutic options across various diseases. Promising candidates include clemastine and amantadine for neurological disorders, digoxin, statins, and aspirin for cancer, minoxidil for androgenic alopecia, and propranolol for infantile hemangioma. These investigations have also revealed the mechanisms through which existing drugs exert effects in new contexts. However, translating these findings into established treatments requires addressing challenges related to assay validity, model relevance, clinical trial design, and the complexity of human disease.
INTRODUCTION
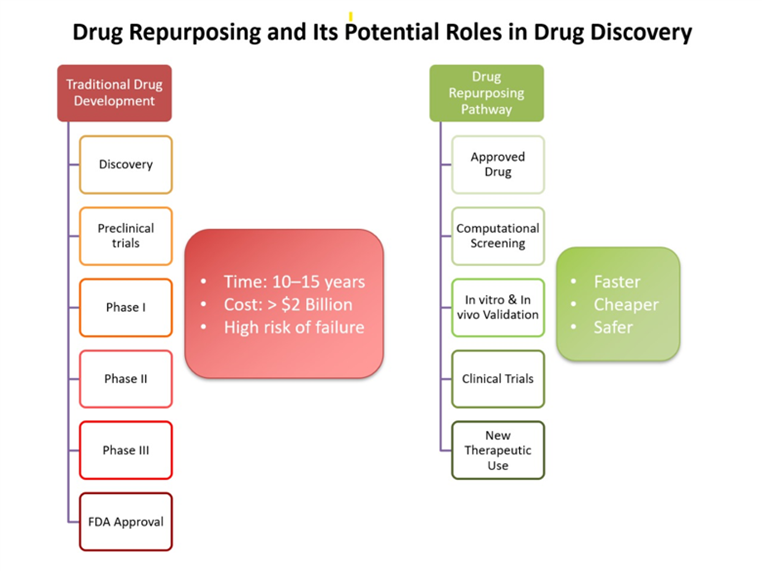
Drug repurposing, also known as drug repositioning, represents an innovative strategy within pharmaceutical development that entails identifying novel therapeutic applications for existing medications. These drugs may exhibit therapeutic efficacy in the treatment of different diseases due to shared pathological pathways, off-target effects, or broader biological activities than initially acknowledged. This approach has gained considerable attraction in recent years as a cost-effective and time-efficient alternative to traditional drug discovery, which frequently necessitates over a decade of extensive research and substantial financial investment (Figure I). The pressing need to identify treatments for rare, complex, or emerging diseases has further emphasized the significance of drug repurposing in contemporary medicine.
METHOD
Drug repurposing can be implemented through several complementary methodologies. Historically, serendipitous clinical observations and off-label usage have played crucial roles in uncovering new indications for existing drugs. In more recent times, systematic methodologies have emerged, employing computational tools such as molecular docking, gene expression profiling, and network pharmacology to predict drug-disease relationships. Experimental strategies, which include in vivo animal studies, and clinical trials, are frequently utilized to validate these computational predictions. Advances in data analytics, access to electronic health records, and the availability of large-scale biological databases have significantly improved the feasibility and accuracy of repurposing initiatives.
Computational drug repositioning methods fall into five main categories:
- Target-based: Identifying new targets for existing drugs using molecular docking (e.g., antivirals screened for cancer proteins).
- Knowledge-based: Using literature and clinical data to find off-label uses (e.g., beta-blockers for anxiety).
- Signature-based: Matching drug-induced gene expression profiles to disease signatures (e.g., CMap for cancer reversal).
- Pathway/network-based: Exploring biological networks to predict new uses (e.g., statins in cancer signaling pathways).
- Mechanism-targeted: Repurposing drugs based on known actions (e.g., propranolol for infantile hemangioma due to anti-angiogenic effects [1][2].
In vitro assays provide distinct advantages in drug repositioning by enabling direct, disease-relevant mechanistic insights, supporting high-throughput screening of diverse compounds across full concentration–response ranges, facilitating hypothesis-free identification of unexpected effects, and generating robust data to guide prioritization for subsequent phenotypic or in vivo evaluations. Examples of these in vitro cells used for drug repurposing include a Chinese hamster ovary (CHO) cell line expressing the amyloid precursor protein 751WT, which is used to test FDA-approved drugs for their possible effects in treating Alzheimer’s disease [3]. Furthermore, many cancer cell lines are used for repurposing drugs to treat various types of cancers, such as prostate cancer cell lines LNCaP and PC3, and the U87 glioblastoma cell line [4][5].
In vivo animal studies are essential in drug repurposing as they validate therapeutic hypotheses in a physiologically relevant system, assessing pharmacokinetics, pharmacodynamics, and safety, and revealing systemic effects and off-target toxicities. These models help optimize dosing and inform clinical trial design, though species differences, ethical concerns, and costs remain key limitations. [6][7]
Clinical trials are crucial in drug repurposing as they provide definitive evidence of safety, efficacy, and optimal dosing in humans. They validate preclinical findings, assess long-term safety, identify adverse effects, and measure clinical endpoints critical for regulatory approval. Despite their cost and complexity, clinical trials remain the cornerstone for translating repurposed drugs into approved therapies. A notable example on the role of clinical trials in drug repurposing is their use in discovering effective treatments against COVID-19 [8], in addition to several examples that will be mentioned in this review.
The advantages associated with drug repurposing are substantial, as repurposed drugs already have established safety profiles and pharmacokinetic data, significantly shortened development timelines and reducing regulatory burdens. This expedited process is particularly beneficial during public health emergencies or for diseases with limited treatment options, such as COVID-19 pandemic.
Furthermore, repurposing may reveal novel therapeutic mechanisms, thereby contributing to a more profound understanding of disease biology. Nonetheless, challenges persist, including intellectual property constraints, the necessity for rigorous validation of efficacy for new indications, and the potential risk of unforeseen adverse effects in diverse patient populations or disease contexts. This review aims to thoroughly examine the current landscape of drug repurposing, concentrating on case studies across various therapeutic domains, including neurology, infectious diseases, oncology, and endocrinology. It underscores both successful and emerging examples, delineates mechanisms of action, and evaluates clinical outcomes, thereby providing valuable insights into the potential and limitations of drug repurposing as a transformative tool in drug discovery and development.
RESULT AND DISCUSSION
Amantadine Repurposed from Antiviral Drug to Treat Neurological Conditions in Patients
As indicated in Table I, numerous studies have investigated the efficacy of amantadine in the treatment of Levodopa-Induced Dyskinesia (LID). The efficacy and safety of amantadine in Parkinson’s Disease with Levodopa-Induced Dyskinesia (EASED) study was a randomized, double-blind, placebo-controlled, parallel-group trial that assessed various doses of ADS-5102 (extended-release amantadine). The primary outcome revealed that a dosage of 340 mg ADS-5102 resulted in a statistically significant reduction in dyskinesia compared to placebo, as measured by the Unified Dyskinesia Rating Scale (UDysRS) total score [9]. The efficacy and safety of amantadine in the treatment of Levodopa-Induced Dyskinesia in Parkinson’s Disease, Phase 3 (EASE LID 3) study further corroborated the efficacy and safety of 274 mg ADS-5102 (equivalent to 340 mg amantadine HCl) for LID. This study also demonstrated enhancements in ON time without troublesome dyskinesia and reductions in OFF time. It is hypothesized that amantadine mitigates the N-methyl-D-aspartate (NMDA) receptor sensitivity of striatal medium spiny neurons to glutamatergic input and inhibits gamma-aminobutyric acid (GABA) release at the substantia nigra [10].
An open-label pilot study investigated the long-term effects of repeated intravenous amantadine infusions in Parkinson’s Disease (PD) patients, both with and without dyskinesias. While substantial immediate improvements in motor scores (Unified Parkinson’s Disease Rating Scale [UPDRS]) were observed post-infusion across both groups, the long-term changes in motor scores over a six-month period were not statistically significant. Nonetheless, in patients exhibiting dyskinesias, a notable improvement in Abnormal Involuntary Movement Scale (AIMS) scores was documented between the initial and final visits. The mechanism underlying these effects is believed to involve reductions in NMDA sensitivity and inhibition of GABA release [11]. A post-hoc analysis of pooled data from two pivotal trials of extended-release amantadine (EASE LID and EASE LID 3) and their open-label extension (EASE LID 2) evaluated the impact of amantadine-ER on OFF-related dystonia in PD patients. The analysis indicated that a 12-week course of extended-release amantadine significantly improved OFF dystonia as assessed by the UDysRS Part 2 and the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) item 4.6. This improvement was maintained over a two-year follow-up and appeared to be independent of reductions in OFF time, with the proposed mechanism involving NMDA receptor antagonism [12]. In addition to its role in Parkinson’s disease, amantadine has exhibited potential in preclinical models of various neurological conditions. In a mouse model of sepsis-associated encephalopathy (SAE), administration of amantadine (30 mg/kg/day, intraperitoneally [i.p.]) resulted in decreased hippocampal levels of the pro-inflammatory cytokine interleukin-1 beta (IL-1β) and enhanced learning and memory capabilities. Notably, this effect was observed even in toll-like receptor 2 (TLR2) knockout mice, suggesting a TLR-independent mechanism—potentially involving the induction of glial cell line-derived neurotrophic factor (GDNF) [13]. In a spinal cord injury (SCI) mouse model, amantadine (2 mg/kg/day i.p.) facilitated neurological recovery by modulating the immune environment. Single-cell RNA sequencing revealed a shift in macrophage subtypes, characterized by a decrease in pro-inflammatory IL-1β-positive inflammatory macrophages (IL-1β+ IMs) and an increase in reparative mannose receptor C-type 1-positive border-associated macrophages (Mrc1+ BAMs) and arginase 1-positive chemotaxis-inducing macrophages (Arg1+ CIMs). This immunomodulation was associated with reduced neuronal apoptosis, an increase in microtubule-associated protein 2-positive (MAP2+) neurons, and improved behavioral and electrophysiological outcomes. Mechanistically, amantadine may exert its effects through the Hypoxia-Inducible Factor-1α (HIF-1α) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathways. These findings underscore the potential of amantadine as a repurposed neuroprotective agent in inflammatory central nervous system (CNS) disorders [14].
Table I. Repurposing of Anti-Viral Medications in Non-Viral Conditions.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Amantadine | Influenza A antiviral | Parkinson’s disease – levodopa-induced dyskinesia | NMDA antagonism; dopaminergic modulation | ADS-5102 ER 340 mg qHS | Randomized controlled trials | ↓ UDysRS; ↑ ON-time without troublesome dyskinesia | [9], [10] |
| Amantadine | Influenza A antiviral | OFF-related dystonia in PD | NMDA antagonism | 137–274 mg ER, 12 weeks | Post-hoc analysis + extension | Improved OFF-related dystonia sustained up to 2 years | [12], [4] |
| Amantadine | Influenza A antiviral | PD motor symptoms (IV exposure study) | NMDA antagonism; reduced glutamatergic drive | 200 mg IV (repeated infusions) | Open-label pilot | Immediate motor improvement; AIMS improvement at 6 months (dyskinesia subgroup) | [11] |
| Amantadine | Influenza A antiviral | Sepsis-associated encephalopathy (preclinical) | Possibly via GDNF; TLR-independent | 30 mg/kg/day i.p. | Mouse in vivo | ↓ hippocampal IL‑1β; improved learning & memory | [13] |
| Amantadine | Influenza A antiviral | Spinal cord injury (preclinical) | HIF‑1α / NF‑κB modulation; macrophage phenotype shift | 2 mg/kg/day i.p. | Mouse in vivo | ↓ inflammatory macrophages; ↑ reparative macrophages; improved BBB score & MEPs | [14] |
PD: Parkinson’s Disease | ADS-5102 ER: Extended-release Amantadine | UDysRS: Unified Dyskinesia Rating Scale | AIMS: Abnormal Involuntary Movement Scale | TLR: Toll-Like Receptor | IL-1β: Interleukin-1 beta | HIF-1α: Hypoxia-Inducible Factor 1-alpha | NF-κB: Nuclear Factor kappa-light-chain-enhancer of activated B cells | BBB score: Basso, Beattie, and Bresnahan locomotor rating scale | MEPs: Motor Evoked Potentials | GDNF: Glial cell line-Derived Neurotrophic Factor
Repurposing Antibacterial Agents for Inflammatory and Non-Infectious Diseases
Repurposing Antibacterial Agents for Rosacea:
As shown in Table II, although antibiotics are conventionally employed to address bacterial infections, numerous studies have investigated their application in non-infectious inflammatory conditions, including rosacea and bronchial asthma [15][16][17].
Rosacea, particularly the papulopustular subtype, is a chronic inflammatory skin condition characterized by persistent facial erythema, papules, and pustules, predominantly affecting the central region of the face. While the precise etiology remains uncertain, it is postulated that rosacea involves a dysregulation of the innate immune response, resulting in increased expression of antimicrobial peptides such as cathelicidin and heightened protease activity, which contribute to inflammation [18].
Beyond its dermatological applications, doxycycline has exhibited potential in preclinical models of tissue repair. In a rat model of deep stromal corneal injury, Chan et al. (2025) assessed a novel doxycycline-loaded gelatin nanoparticle (DNP) formulation aimed at enhancing ocular retention and therapeutic efficacy [19]. The DNP-treated group exhibited accelerated recovery of corneal thickness, improved epithelial healing, reduced stromal thickening, and decreased levels of matrix metalloproteinases (MMP-2 and MMP-9), neutrophil infiltration, and neovascularization ‒ all achieved at a lower dosage and application frequency. These findings underscore the therapeutic promise of doxycycline beyond its antimicrobial role through enhanced drug delivery and anti-inflammatory effects [19].
In a randomized controlled trial lasting 12 weeks, modified-release doxycycline (30 mg immediate release / 10 mg delayed release) was found to significantly reduce inflammatory lesions in patients with papulopustular rosacea compared to a placebo. This clinical improvement was correlated with diminished expression of cathelicidin and protease activity, thereby supporting the anti-inflammatory mechanism of action of doxycycline, which operates independently of its antimicrobial properties [20].
Repurposing Antibacterial Agents for Asthma:
Furthermore, a randomized controlled trial evaluated the efficacy of oral azithromycin as an adjunct to standard therapy in children with poorly controlled asthma. The study reported significant improvements in Asthma Control Test (ACT) scores, enhanced asthma management according to Global Initiative for Asthma (GINA) guidelines, and a reduction in the frequency of exacerbations. These outcomes are likely attributable to the immunomodulatory properties of azithromycin, which contribute to the attenuation of airway inflammation and bronchial hyperresponsiveness [21].
Repurposing Antibacterial Agents for Brain Injury:
In support of its immunomodulatory potential, Barks et al. (2019) explored the neuroprotective efficacy of azithromycin in a neonatal rat model of hypoxic-ischemic brain injury. Administration of azithromycin post-injury resulted in a significant reduction in brain damage and an improvement in sensorimotor function in a dose-dependent manner, with a multi-dose regimen proving more effective than a single dose. The treatment was well tolerated and associated with decreased tissue loss in critical brain regions. Mechanistically, the effects of azithromycin were attributed to the modulation of myeloid cells, specifically promoting anti-inflammatory M2 macrophage phenotypes, thus suggesting its potential as a neuroprotective agent through non-antibiotic mechanisms [22].
Antifungal Agents: Repurposing Applications Beyond Mycology
As shown in Table III, antifungal agents, in particular, have exhibited potential beyond their conventional use in treating infectious diseases, with applications extending into oncology, antibacterial therapy, parasitic diseases, and neuroprotection.
Itraconazole in Cancer
A pre-operative, window-of-opportunity trial examined the effects of fixed-dose oral itraconazole in early-stage non-small cell lung cancer (NSCLC). In this trial, patients received a daily dosage of 600 mg of itraconazole for a duration of 7–10 days prior to surgical resection [23][24]. Plasma and intra-tumoral itraconazole concentrations exhibited considerable variability among patients and were significantly correlated with alterations in tumor volume, perfusion, angiogenic cytokine levels, and microvessel density. Itraconazole is recognized for its antiangiogenic properties, potentially through the inhibition of vascular endothelial growth factor receptor 2 (VEGFR2) glycosylation, trafficking, and signaling [24].
Table II. Repurposing of Antibacterial Medications in Non-Bacterial Conditions.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Doxycycline (DNP) | Antibacterial | Corneal deep stromal wound healing (preclinical) | MMP inhibition; enhanced ocular retention via nanoparticles | DNP 0.01% bid (rats); comparators: topical/oral | Rat in vivo | Faster epithelial/stromal healing; ↓ neovascularization; superior to topical/oral at lower dose | [19] |
| Doxycycline | Antibacterial | Papulopustular rosacea | Inhibits MMPs; anti-inflammatory | 40 mg MR qd | Randomized controlled trial | ↓ inflammatory lesions; improved global assessment; ↓ cathelicidin/protease activity | [20] |
| Azithromycin | Antibacterial | Poorly controlled asthma in children | Immunomodulation; ↓ airway inflammation | 10 mg/kg tiw for 3 months | Randomized controlled trial | ↑ ACT/CACT scores; fewer exacerbations; no spirometry change | [21] |
| Azithromycin | Antibacterial | Neonatal hypoxic‑ischemic brain injury (preclinical) | Myeloid cell modulation; promotes M2 phenotype | Multi‑dose regimen post‑injury | Neonatal rat in vivo | ↓ brain damage; improved sensorimotor function; dose- and timing-dependent efficacy | [22] |
MR: Modified-release | MMPs: Matrix Metalloproteinases | ACT: Asthma Control Test | CACT: Childhood Asthma Control Test | M2 phenotype: Macrophage 2 phenotype | DNP: Doxycycline-Loaded Gelatin Nanoparticles.
Table III. Repurposing of Antifungal Medications in Non-Fungal Conditions.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Itraconazole | Antifungal | Non-small cell lung cancer (pre-op window) | Anti‑angiogenic; affects VEGFR2 trafficking/signaling | 600 mg/day for 7–10 days | Clinical window trial | ↓ tumor perfusion/volume; ↓ angiogenic cytokines; ↓ microvessel density | [23][24] |
| Amphotericin B (liposomal) | Antifungal | Disseminated leishmaniasis | Targets Leishmania membrane sterols | Total 17–37 mg/kg | Clinical (patients with DL) | Cure rate 65–75% depending on dose | [26] |
| Amphotericin B | Antifungal | MRSA (in vitro antibacterial activity) | Binds PBP2a sites; affects conformational stability | MIC 16 μg/mL; MBC 32 μg/mL | In vitro + in silico | Complete growth inhibition at 32 μg/mL; strong docking to PBP2a | [25] |
| L-ketoconazole | Antifungal enantiomer | Cushing’s syndrome (incl. DM subgroup) | Inhibits steroidogenic CYPs (17α‑, 11β‑hydroxylase, SCC) | 150–600 mg bid | Phase 3, open‑label (SONICS) | Normalization of mUFC; ↓ HbA1c & FBG in DM subgroup; improved cardiometabolic markers | [27], [28] |
| Fluconazole | Antifungal | Neuroprotection (preclinical) | IGF‑1R upregulation/signaling → ↓ cAMP; ↑ Akt phosphorylation | In vitro 1–10 μM; in vivo 20 mg/kg | Cells + mouse in vivo | Prevents neuronal death/degeneration; promotes NPC proliferation & neurogenesis | [29] |
MIC: Minimum Inhibitory Concentration | MBC: Minimum Bactericidal Concentration | PBP2a: Penicillin-Binding Protein 2a | mUFC: Mean Urinary Free Cortisol | DM: Diabetes Mellitus | IGF-1R: Insulin-like Growth Factor 1 Receptor | cAMP: Cyclic Adenosine Monophosphate | Akt: Protein Kinase B | NSCLC: Non-Small Cell Lung Cancer
Amphotericin B Against MRSA
Amphotericin B (AMPH), a broad-spectrum antifungal, has been investigated for its antibacterial potential against Methicillin-Resistant Staphylococcus aureus (MRSA). Resistance in MRSA primarily arises from the expression of Penicillin-Binding Protein 2a (PBP2a), which diminishes the efficacy of β-lactam antibiotics. In vitro screening revealed that AMPH demonstrated significant activity against clinical MRSA isolates, with Minimum Inhibitory Concentrations (MIC) of 16 µg/mL and Minimum Bactericidal Concentrations (MBC) of 32 µg/mL [25]. Molecular docking and simulation analyses indicated that AMPH binds to active site of C-terminal transpeptidase domain and the non-penicillin-binding allosteric domain of PBP2a. These interactions influence the protein’s conformational stability, thereby suggesting a mechanism for its antibacterial activity [26].
Liposomal Amphotericin B in Leishmaniasis
Another study assessed the application of liposomal amphotericin B for the treatment of disseminated leishmaniasis (DL). This formulation is specifically designed to enhance drug delivery while minimizing toxicity. The antifungal action of amphotericin B is mediated through its binding to ergosterol in fungal membranes, leading to cell death. In the context of leishmaniasis, amphotericin B targets the membrane of the Leishmania parasite, demonstrating efficacy in patients with DL. The study provides clinical evidence supporting its utilization as a repurposed agent for parasitic infections [25, 26].
L-ketoconazole in Cushing’s Syndrome and Diabetes Mellitus
L-ketoconazole, the 2S,4R enantiomer of ketoconazole, was evaluated in the SONICS phase 3 study for the treatment of Cushing’s syndrome. This multicentre, open-label, single-arm clinical trial involved participants receiving L-ketoconazole during both a dose-titration and a maintenance phase. In the overall study population, the drug effectively reduced and normalized mean urinary free cortisol concentrations [27][28]. Among a subgroup of 28 patients with diabetes mellitus (DM), significant reductions in fasting blood glucose and HbA1c levels from baseline were observed by the conclusion of the maintenance phase. Additionally, changes in antidiabetic medication utilization were reported, with some patients requiring new medications, dose adjustments, or discontinuation of previous therapies. L-ketoconazole exerts its effects by potently inhibiting several enzymes involved in steroidogenesis, including 17α-hydroxylase, 11β-hydroxylase, and cholesterol side-chain cleavage enzymes, thereby diminishing cortisol synthesis [27][28].
Fluconazole in Neuroprotection
Fluconazole, a widely utilized antifungal agent, has exhibited neuroprotective properties in both in vitro and in vivo models. Experimental investigations involving neuronal and neural progenitor cells, along with mouse models of neurotoxicity, have demonstrated that fluconazole can prevent neuronal death, inhibit neuronal degeneration, and promote neural progenitor cell proliferation and neurogenesis [29]. These protective effects have been observed against multiple neurotoxic challenges, including oxidative stress (3-Nitropropionic acid, 3-NOPA), excitotoxicity (N-Methyl-D-aspartate, NMDA), dopamine toxicity (6-Hydroxydopamine, 6-OHDA), and HIV-1 proteins (Tat and gp120). The proposed mechanism involves fluconazole’s interaction with the Insulin-like Growth Factor 1 Receptor (IGF-1R). The drug enhances IGF-1R expression and activates its signaling pathway, resulting in decreased intracellular cyclic adenosine monophosphate (cAMP) levels and increased phosphorylation of protein kinase B (Akt). This signaling cascade supports neuronal survival and inhibits apoptosis. Inhibition of IGF-1R signaling has been shown to obstruct these effects, suggesting that fluconazole may function as an IGF-1R agonist [29]. However, translating these findings into clinical practice requires pharmacokinetic and safety validation in humans at doses relevant for neuroprotection. Targeted trials are needed to confirm efficacy in specific neurological conditions such as Alzheimer’s disease, Parkinson’s disease, or HIV-associated neurocognitive disorders. Mechanistic confirmation in human tissues is necessary to ensure IGF-1R agonism is consistent and does not produce off-target effects. In summary, fluconazole’s established safety profile and oral bioavailability make it an attractive candidate for repurposing, but rigorous clinical trials and mechanistic studies are essential before therapeutic adoption.
Antidiabetic Medications Repurposed to Treat Neurological Problems
As demonstrated in Table IV, earlier research has extensively examined the GLP-1 counterpart liraglutide in Alzheimer disease (AD) models. In 5xFAD mice, chronic liraglutide therapy (25 nmol/kg/day, equivalent to 0.0938 mg/kg/day, subcutaneously for 8 weeks) improved mitochondrial activity, prevented neuron loss, and activated the cAMP/PKA pathway [30]. This was associated with higher cAMP and p-PKA levels in the brain. The AD mouse model accelerated cell growth and differentiation into neurons, thus it is beneficial in neurodegenerative diseases like AD [30, 31]. In the same context, DPP-4 inhibitor has demonstrated encouraging outcomes in AD models. In 9-month-old 3xTg-AD mice, oral linagliptin (5, 10, and 20 mg/kg for 8 weeks) enhanced learning and memory as measured by the Y-maze and Morris Water Maze. Increased incretin levels that crossed the blood-brain barrier as a result of peripheral DPP-4 inhibition were linked to this cognitive improvement. By inhibiting IRS-1 (s307) and addressing AD-related issues in hippocampus neurons of Aβ (1-42) infused rats, linagliptin treatment significantly reduced brain insulin resistance (given orally at 0.513 mg/kg, 3 mg/kg, and 5 mg/kg for 8 weeks) [32][33]. This was accompanied by reversed motor and cognitive impairment, elevated GLP-1 levels, and diminished soluble Aβ (1–42), IRS-1 (s307), GSK-3β, pro-inflammatory cytokines (TNF-α, IL-1β, IL-6), acetylcholinesterase (AChE) activity, and oxidative/nitrosative stress in the hippocampus. Histopathological investigation (H&E and Congo red staining) revealed that linagliptin has neuroprotective and anti-amyloidogenic properties [32][33].
Table IV. Repurposing of Anti-Diabetic Drugs.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Liraglutide (GLP‑1 analogue) | Type 2 diabetes | Alzheimer’s disease (models) | GLP‑1R activation → cAMP/PKA; Akt/GSK‑3β modulation | 25 nmol/kg/day s.c. (mice) | Mouse in vivo | ↑ neurogenesis; ↓ tau phosphorylation; improved mitochondrial dynamics & cognition | [30], [31], |
| Linagliptin (DPP‑4 inhibitor) | Type 2 diabetes | Alzheimer’s disease (models) | ↑ incretins crossing BBB; restores insulin signaling; anti‑inflammatory/antioxidant | 5–20 mg/kg oral (mice/rats) | Mouse/rat in vivo | Improved memory; ↓ Aβ42, tau‑P, IRS‑1(s307), cytokines; ↑ hippocampal GLP‑1 | [32], [33] |
| Pioglitazone + Leptin | Type 2 diabetes (pioglitazone); hormone (leptin) | Alzheimer’s disease (model) | PPAR‑γ agonism + leptin neuroprotection | Pioglitazone 10 mg/kg i.p.; Leptin 0.03 mg/kg intranasal | Mouse in vivo | Improved spatial memory; ↓ Aβ burden; ↓ neuroinflammation | [34] |
| Pioglitazone SR | Type 2 diabetes | Delay MCI due to AD (high‑risk adults) | PPAR‑γ agonism | 0.8 mg once daily (SR) | Phase 3 RCT | No significant delay in MCI onset vs placebo (TOMMORROW) | [35] |
| Rosiglitazone | Type 2 diabetes | Neuroinflammation/AD‑related changes (model) | PPAR‑γ agonism; NF‑κB inhibition | 1–5 mg/kg | Rat in vivo | ↓ Aβ, GFAP, inflammatory and oxidative markers; improved learning/memory | [36] |
| SGLT2 inhibitors (class) | Type 2 diabetes | Cognitive outcomes (longitudinal human data) | ↓ glucotoxicity; neurovascular protection (hypothesized) | Real‑world use ≥3 years | Observational longitudinal | ↑ RBANS total & language domain scores vs non‑users | [37] |
GLP-1: Glucagon-Like Peptide-1 | cAMP: Cyclic Adenosine Monophosphate | Akt: Protein Kinase B | | DPP-4: Dipeptidyl Peptidase-4 | BBB: Blood-Brain Barrier | Aβ42: Amylod Beta 42 | GSK-3β: Glycogen Synthase Kinase-3 beta | PPAR‑γ: Peroxisome Proliferator-activated Receptor Gamma | MCI: Mild Cognitive Impairment | IRS-1 (s307): Insulin Receptor Substrate-1 serine 307 | RBANS: Repeatable Battery for the Assessment of Neuropsychological Status | GFAP: Glial Fibrillary Acidic Protein | TNF-α: Tumor Necrosis Factor-alpha | IL-6: Interleukin-6 | SGLT2: Sodium-Glucose Cotransporter
Pioglitazone and rosiglitazone, PPAR-γ agonists used in type 2 diabetes mellitus (T2DM), have been studied in Alzheimer’s models. A clinical research study (TOMMORROW study extension) that used oral pioglitazone SR (0.8 mg once day) in those at high risk of developing Alzheimer’s disease found that it did not significantly delay the onset of moderate cognitive impairment when compared to placebo [34][35]. However, the study successfully resolved recruitment and implementation issues in this asymptomatic population. Pioglitazone has been found in preclinical studies to be effective in a mouse model of Alzheimer’s disease when combined with leptin. A 2-week therapy with intranasal leptin (0.03 mg/kg/day) and intraperitoneal pioglitazone (10 mg/kg/day) in 6-month-old APP/PS1 mice improved spatial memory deficits (Y maze) and reduced brain β-amyloid levels (soluble and plaque burden). The combination therapy also improved plaque-associated neuritic disease and synapse loss while reducing neocortical glial response [34]. Furthermore, in a rat model of LPS-induced neuroinflammation, rosiglitazone (1, 3, or 5 mg/kg administered 30 mins before LPS for two weeks) reversed elevated levels of Aβ and GFAP in the hippocampus, as well as neuroinflammation and oxidative stress markers. Rosiglitazone also improved LPS-induced learning and memory deficit in the Morris water maze and passive avoidance tests [36].
Furthermore, longitudinal research involving 476 individuals with T2DM, with a follow-up time of up to 6.4 years, investigated the relationship between SGLT2 inhibitor use and changes in cognitive function as measured by the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). The study found that long-term usage of SGLT2 inhibitors for three years or more was linked with a higher RBANS total score (coefficient 0.54; 95% CI 0.13-0.95; p = 0.010) and specifically within the language domain. This beneficial correlation remained significant even after accounting for demographic, clinical, and medication-related variables. Notably, there was no significant cognitive loss in immediate memory or language areas between SGLT2 inhibitor users and non-users in this group. The SGLT2 inhibitors utilized in this real-world trial were canagliflozin, dapagliflozin, and empagliflozin. The observed beneficial correlation between long-term SGLT2 inhibitor use and cognitive function, notably in the language domain, could be attributed to reduced glucotoxicity in the brain and protective effects of these drugs on the neurovascular unit [37].
The language domain evaluation in RBANS includes activities that indicate executive function, a cognitive domain known to be compromised in T2DM and associated with cerebral microvascular damage. By lowering hyperglycemia, SGLT2 inhibitors may help maintain the integrity and function of the neurovascular unit, potentially minimizing cognitive deterioration. These findings imply that SGLT2 inhibitors may have a role in reducing cognitive impairment in T2DM patients, necessitating more research through randomized controlled trials to confirm their potential as disease-modifying therapy [37].
Collectively, these findings suggest that antidiabetic agents, through mechanisms such as enhancing incretin signalling, reducing insulin resistance, and mitigating neuroinflammation, may exert disease-modifying effects in neurodegenerative disorders, offering a promising therapeutic avenue beyond glycemic control.
Central Nervous System Medications Repurposing
Table V lists a number of drug repurposing candidates that have been studied for possible therapeutic uses in other conditions. Selective serotonin reuptake inhibitors (SSRIs), such as dapoxetine and paroxetine, were studied for the treatment of premature ejaculation (PE). According to a meta-analysis by Yue et al., dapoxetine (30 mg or 60 mg as needed) was more effective than placebo in lengthening ejaculatory latency duration in adult males with PE [38, 39].
Similarly, Abu El-Hamd and Abdelhamed [39] found that a combination of sildenafil and paroxetine (30 mg as needed) resulted in significantly greater Premature Ejaculation Diagnostic Tool (PEDT) scores than other groups in humans with PE. Their mechanism is based on blocking serotonin reuptake, which affects brain circuits involved in ejaculation. Moreover, Zhang et al. [40] investigated domperidone, a medication known to elevate serum prolactin, in humans with relapsing-remitting multiple sclerosis (RRMS). It improved MRI texture dissimilarity and fractional anisotropy at 16 and 32 weeks while dramatically increasing serum prolactin levels when given 10 mg three times a day for 16 weeks. The explanation is based on animal research showing that prolactin has the capacity to stimulate remyelination. The medicine was reported to be well tolerated, with no major side effects.
Table V. Repurposing of Central Nervous System Drugs.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Dapoxetine | Premature ejaculation (on‑label for PE in some regions) | — (repurposing context: SSRI use for PE) | SSRI – serotonin reuptake inhibition | 30 or 60 mg prn | Meta‑analysis of RCTs | Prolonged IELT vs placebo; improved patient‑reported outcomes | [38] |
| Paroxetine ± Sildenafil | Depression (original); PE (off‑label repurposing) | Premature ejaculation | SSRI; with PDE5 inhibitor synergy | Paroxetine 30 mg prn ± sildenafil | Randomized clinical trial | Combination outperformed monotherapies by PEDT | [39] |
| Domperidone | Antiemetic / prokinetic | Relapsing‑remitting MS (remyelination adjunct) | ↑ Prolactin → remyelination (preclinical rationale) | 10 mg t.i.d. for 16 weeks | Pilot randomized controlled trial | Improved MRI lesion texture & FA; increased serum prolactin; well tolerated | [40] |
| Memantine | Alzheimer’s disease | Adult ADHD (EF deficits) | Uncompetitive NMDA antagonist; modulates glutamate/dopamine | Up to 10 mg bid | Pilot RCT | Trend improvements in inhibition/self‑monitoring; overall cognition not significantly changed | [41] |
| Gabapentin (G‑GR & others) | Antiepileptic/ neuropathic pain | PHN / pediatric neuropathic pain / radiculopathy | α2δ‑1 VGCC subunit binding → ↓ excitatory neurotransmitters | 300–3600 mg/day (varies) | Multiple RCTs | Reduced pain & sleep interference; mixed non‑inferiority vs fentanyl; tolerability varies | [42][43][44][45] |
| Levetiracetam | Antiepileptic | Glioblastoma chemo-radiosensitizer | Enhances p53‑mediated MGMT suppression | Up to 2000 mg/day | Open‑label phase 2 | ↑ 6‑mo PFS & 24‑mo OS vs external controls; greater benefit <65 y or unmethylated MGMT | [46] |
| Valproic acid | Antiepileptic | Recurrent/metastatic HNSCC (combo) | HDAC inhibition → EMT reversal; chemo-sensitization | Titrate to 50–100 µg/mL | Phase II combination study | Well tolerated with cisplatin + cetuximab; aimed to improve ORR | [47] |
| Clemastine | Antihistamine | Remyelination (MS models); safety cardiac | Antimuscarinic; Notch‑1 modulation; hERG inhibition risk | 5 mg/kg/day (preclinical); IV high‑dose safety signals | Preclinical + proarrhythmia model | Improved remyelination & behavior in EAE; QT prolongation at supratherapeutic IV doses | [48], [49] |
| Fluphenazine | Antipsychotic | Breast cancer (in vitro) | Induces cuproptosis via FDX1↑; copper‑dependent death | 10–20 µM (in vitro) | Cell lines in vitro | ↓ viability; ↓ clonogenic survival; > disulfiram potency in assays | [50] |
RCT: Randomized Controlled Trial | IELT: Intravaginal Ejaculatory Latency Time | PEDT: Premature Ejaculation Diagnostic Tool | FA: Fractional Anisotropy | ADHD: Attention-Deficit/Hyperactivity Disorder | EF: Executive Function | G-GR: Gastroretentive Gabapentin | PHN: Postherpetic Neuralgia | VGCC: Voltage-Gated Calcium Channel | PFS: Progression-Free Survival | OS: Overall Survival | HDACi: Histone Deacetylase Inhibitor | MGMT: O6-Methylguanine-DNA Methyltransferase | HNSCC: Head and Neck Squamous Cell Carcinoma | EMT: Epithelial-Mesenchymal Transition | ORR: Overall Response Rate | MS: Multiple Sclerosis | hERG: Human ether-à-go-go-Related Gene | EAE: Experimental Autoimmune Encephalomyelitis | FDX1: Ferredoxin 1
In addition, Biederman et al. [41] studied the efficacy of memantine, an uncompetitive NMDA receptor antagonist used to treat Alzheimer’s disease, for executive function deficits in adult attention defect hyperactivity disorders (ADHD) patients. It exhibited improvements in specific executive functions (inhibition and self-monitoring) but no meaningful improvement in total cognitive performance when dosed at 5 mg/day and increased to 10 mg twice daily. Suggested mechanisms involves controlling glutamate activity in the prefrontal cortex, preventing excitotoxicity, and affecting dopamine activity.
Moreover, gabapentin, an anticonvulsant that binds to the alpha2-delta subunit of presynaptic voltage-gated calcium channels, has been used in numerous studies for pain management. For postherpetic neuralgia (PHN), Kantor et al. [42] discovered that once-daily gabapentin (300–3600 mg/day) was both efficacious and well-tolerated, lowering pain levels and enhancing quality of life. Brown et al. [43] showed that both amitriptyline (10 mg) and gabapentin (900 mg/day) had similar effects in decreasing pain intensity scores and improving sleep when compared in children with neuropathic pain and complicated regional pain syndrome type I. A previous study [44] compared duloxetine (30–60 mg daily) and gabapentin (300–900 mg/day) for painful diabetic peripheral neuropathy and found that pain severity levels were considerably lowered by both medications. Both worked well to reduce pain and interfere with sleep; however, gabapentin had more adverse effects and worse compliance than duloxetine, although providing quicker immediate relief. A study comparing gabapentin (up to 2400 mg/day) with transdermal fentanyl (up to 100 mcg/h) for persistent neuropathic pain of radicular origin (lumbar radiculopathy) was carried out [45]. After 56 days, there were no statistically significant variations in the level of pain.
Furthermore, levetiracetam, an anti-epileptic drug primarily used for seizure management, has been investigated for its potential role as a chemosensitizer in glioblastoma treatment. In an open-label phase 2 study, Hwang et al. reported that levetiracetam, titrated up to 2000 mg/day, improved 6-month progression-free survival and 24-month overall survival compared to external controls. The benefit was more pronounced in patients under 65 years or with unmethylated MGMT promoters. Mechanistically, levetiracetam may enhance p53-mediated suppression of MGMT expression, thereby increasing tumor sensitivity to temozolomide chemotherapy [46]. Similarly, valproic acid (VPA), an anti-epileptic drug with histone deacetylase inhibitor (HDACi) activity, has been repurposed for oncology applications. In the V-CHANCE trial, VPA was combined with cetuximab and cisplatin for recurrent or metastatic head and neck squamous cell carcinoma (HNSCC), with titration to achieve serum levels of 50–100 µg/mL. Its HDACi activity is proposed to reverse epithelial–mesenchymal transition (EMT), enhance tumor chemosensitivity, and modulate gene expression. Although originally a CNS-acting medication, VPA’s repurposing leverages non-CNS mechanisms to target systemic cancer [47].
In the same context., clemastine, a first-generation antihistamine with anticholinergic and antimuscarinic properties, is being explored for remyelination and cardiac safety. Kawakami et al. [48] reported that while low and moderate intravenous doses (0.03–0.3 mg/kg) had minimal cardiac effects, a high supratherapeutic dose (3 mg/kg) significantly prolonged QT and MAP90 intervals and induced arrhythmias, likely via hERG K⁺ channel inhibition. Conversely, Ibrahim et al. demonstrated that oral clemastine (5 mg/kg/day) improved sensory and motor function, reduced neuroinflammation, and enhanced remyelination in an EAE rat model. Mechanistically, clemastine promotes oligodendrocyte differentiation by modulating Notch-1 signalling and suppressing astrocyte and microglial activation [48][49].
Moreover, fluphenazine, a first-generation antipsychotic, has demonstrated potential anti-cancer activity through a novel mechanism. In silico screening using CMap and TCGA databases and in vitro studies using breast cancer cell lines (MCF-7, MDA-MB-453, MDA-MB-231) confirmed its anticancer efficacy. It significantly reduced cell viability and clonogenic survival by inducing cuproptosis, a copper-dependent cell death pathway at concentrations of 10–20 µM. This effect was associated with upregulation of FDX1, increased intracellular copper, and decreased pyruvate accumulation, and was reversed by inhibitors of mitochondrial pyruvate transport (UK5099) or cuproptosis (penicillamine). Notably, fluphenazine outperformed disulfiram, another cuproptosis inducer, highlighting its promise as a repurposed anti-cancer agent despite its original CNS indication [50].
Drugs Used to Treat Gastrointestinal Illnesses Can be Repurposed to Treat Other Diseases Several gastrointestinal (GIT) drugs have been repurposed for non-GIT indications. In a randomized trial, combined antihistamines (desloratadine 2.5 mg and ranitidine 75 mg twice daily) reduced allergic reactions in children with peanut allergy but caused neuropsychiatric symptoms without improving quality of life, likely via H1/H2 receptor blockade [51]. Intranasal scopolamine (0.2–0.4 mg) significantly increased motion sickness tolerance in healthy adults without major cognitive effects, acting as a muscarinic cholinergic antagonist [52]. Oral domperidone (60 mg/day for 14 days) enhanced breast milk production and prolactin levels in mothers with lactation failure through dopamine receptor antagonism [53]. For pain in cutaneous ulcers, topical morphine and loperamide (10 mg each) were both effective, mediated by peripheral μ-opioid receptor activation [54]. Additionally, lubiprostone improved serotonin signalling and motility in rats by stimulating EP1/EP4 receptors [55], while omeprazole demonstrated antidepressant-like effects in mice by inhibiting serotonin synthesis (TPH1/TPH2) and degradation (MAO-A), increasing brain serotonin levels [56].
Cardiovascular System Medications Can Be Repurposed to Treat Cancer
Cardiovascular drugs show significant potential for repurposing in diverse conditions. Aspirin, a widely used NSAID, has demonstrated anti-cancer effects in breast and lung
malignancies. Evidence from clinical and preclinical studies indicates that aspirin (81 mg daily for prevention or 325 mg daily for therapeutic use) can suppress metastasis, inhibit tumor growth, and prevent recurrence through COX enzyme inhibition and anti-inflammatory mechanisms, with added potential in combination regimens [57].
Similarly, digoxin, a cardiac glycoside traditionally used for heart failure, exhibited anti-tumor effects in in vitro studies on NSCLC cell lines and in vivo xenograft models, reducing metastasis and enhancing chemotherapy efficacy via Na⁺/K⁺-ATPase inhibition and calcium-mediated signaling at doses of 0.25–1 mg/day [58].
Other CVS drugs have been repurposed for non-cancer indications based on clinical trial evidence. Minoxidil, an antihypertensive agent, improved hair density in androgenetic alopecia when administered orally (5 mg/day), likely by activating potassium channels and increasing scalp blood flow, with minimal cardiovascular impact [59]. Propranolol, a beta-blocker, achieved significant regression of infantile hemangiomas (3 mg/kg/day for 6 months) by inhibiting angiogenesis and vasodilation [60].
Additionally, statins (e.g., simvastatin, atorvastatin, fluvastatin, pravastatin, rosuvastatin, lovastatin) have been explored for cancer therapy at doses of 20–80 mg/day. While clinical trial outcomes vary, preclinical studies consistently report decreased proliferation, enhanced apoptosis, and inhibition of metastasis. Mechanisms include mevalonate pathway inhibition, NF-κB suppression, caspase activation, and modulation of cell cycle regulators, with potential synergy when combined with immunotherapy or chemotherapy [61][62].
Repurposing of Antihistamine Drugs
Antihistamines have shown promising repurposing potential beyond their traditional uses. In silico molecular docking techniques explored the potential of H1 antihistamines in inhibiting RNA-dependent RNA polymerase (RdRp), a key enzyme involved in viral replication, thus combating COVID-19 [63]. In this context, both in silico and in vitro approaches explored the potential anti-influenza activity of cyproheptadine, a clinically used histamine H1 receptor antagonist. The in-silico study revealed the similarity between cyproheptadine and several established anti-influenza agents, and further experimental in vitro evaluation demonstrated its anti-influenza activity [64]. Clinical evidence provided by Koh et al. [65] evaluated chlorcyclizine (75 mg twice daily) for chronic HCV infection; while monotherapy was ineffective, combination with ribavirin achieved >3-fold reductions in HCV RNA in 58% of patients, suggesting a synergistic antiviral effect via inhibition of late-stage viral entry. Moreover, Matsushita et al. [66] investigated meclizine (12.5–25 mg/day) in children with achondroplasia, reporting good tolerability and steady-state plasma levels, supporting its potential as a bone growth therapy through FGFR3 signalling blockade. Another clinical study performed by El-Fatatry et al. who studied fexofenadine (60 mg/day) combined with ramipril in diabetic kidney disease. The researchers observed significant reductions in albuminuria and preservation of eGFR, likely mediated by anti-inflammatory and antioxidant effects, indicating renal protection [67]. Collectively, these findings highlight the versatility of antihistamines as candidates for drug repurposing. Their established safety profiles, diverse pharmacological actions, and demonstrated efficacy in clinical and experimental settings underscore their potential to address unmet therapeutic needs beyond traditional indications
Table VI. Repurposing of Gastrointestinal Drugs.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Desloratadine + Ranitidine | Allergic conditions / acid suppression | Premedication in peanut OIT (children) | H1/H2 blockade | Desloratadine 2.5 mg + Ranitidine 75 mg bid | Randomized clinical trial | ↓ moderate–severe reactions but ↑ neuropsychiatric effects; no QoL gain | [51] |
| Intranasal Scopolamine | Antimuscarinic (motion sickness) | Motion sickness tolerance (healthy adults) | Muscarinic blockade of vestibular input | 0.2–0.4 mg intranasal | Randomized, double‑blind, placebo‑controlled | ↑ motion sickness tolerance; no major cognitive deficits | [52] |
| Domperidone | Prokinetic/ antiemetic | Lactation failure (milk production) | D2 antagonism → ↑ prolactin | 10 mg, 2 tabs t.i.d. × 14 days | Randomized, double‑blind, placebo‑controlled | ↑ exclusive breastfeeding at day 7; no long‑term difference; safe | [53] |
| Topical Morphine or Loperamide | Analgesia / antidiarrheal | Pain in dermal ulcers | Peripheral µ‑opioid receptor activation | 10 mg topical (each) with gel | Randomized crossover | Both reduced pain; better satisfaction with morphine; no systemic effects | [54] |
| Lubiprostone | Constipation (CF-related GI phenotype) | CF mouse intestinal phenotype | Activates ClC‑2 channels → ↑ fluid secretion | 10 µg/kg/day × 2 weeks (gavage) | Mouse in vivo | ↓ bacterial overgrowth; ↑ gastric emptying; mixed effects on mucus/ transit | [55] |
| Omeprazole | Proton pump inhibitor | Antidepressant‑like effects (preclinical) | Inhibits TPH1/TPH2 & MAO‑A → ↑ 5‑HT availability | 100 mg/kg/day × 4 days (mice) | In vitro + mouse in vivo | ↑ brain/serum 5‑HT; ↓ immobility in TST | [56] |
OIT: Oral Immunotherapy | QoL: Quality of Life | CF: Cystic Fibrosis | CIC-2: Chloride Channel 2 | 5-HT: Serotonin | TPH1: Tryptophan Hydroxylase 1 | TPH2: Tryptophan Hydroxylase 2 MAO-A: Monoamine Oxidase A | TST: Tail Suspension Test
Table VII. Repurposing of Cardiovascular drugs.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Aspirin | Analgesic/ antiplatelet | Breast & lung cancers (varied settings) | COX inhibition; anti‑inflammatory; anti‑metastatic pathways | 81–325 mg/day (context dependent) | Preclinical + clinical studies | ↓ tumor growth/metastasis; recurrence prevention; potential synergy in combination | [57] |
| Digoxin | Heart failure/ arrhythmias | Non‑small cell lung cancer | Na+/K+‑ATPase inhibition → Ca2+ signaling affecting proliferation | 0.25–1 mg/day (context dependent) | In vitro + in vivo xenografts | ↓ tumor growth/metastasis; ↑ chemotherapy efficacy; reduced adriamycin cardiotoxicity | [58] |
| Minoxidil | Antihypertensive | Androgenetic alopecia (hair growth) | K+ channel opener; ↑ scalp blood flow | 5–7.5 mg/day oral | Clinical monitoring/observational | ↑ hair density; ↑ heart rate without BP change (Holter/ABPM) | [59] |
| Propranolol | Beta‑blocker | Infantile hemangioma | Anti‑angiogenic; vasoconstrictive; anti‑proliferative | 3 mg/kg/day × 6 months | Randomized controlled trial | Significant regression; well tolerated | [60] |
| Statins (class: simvastatin/atorvastatin/etc.) | Dyslipidemia | Various cancers (gynecologic, others) | Mevalonate pathway inhibition; NF‑κB↓; apoptosis↑; EMT↓ | 20–80 mg/day (drug‑specific) | Preclinical + clinical (mixed) | ↓ proliferation; ↑ apoptosis; variable clinical outcomes; synergy with chemotherapy/immunotherapy | [61], [62] |
NSAID: Non-Steroidal Anti-Inflammatory Drug | NSCLC: Non-Small Cell Lung Cancer | COX: Cyclooxygenase | Na+/K+-ATPase: Sodium/Potassium Adenosine Triphosphatase | AMPK: AMP-Activated Protein Kinase | EMT: Epithelial-Mesenchymal Transition | PTTG1: Pituitary Tumor-Transforming Gene 1 | p21/p27: Cyclin-Dependent Kinase Inhibitors.
Table VIII. Repurposing of Antihistamine Drugs.
| Drug Name | Original Indication | Repurposed Indication | Mechanism of Action | Dose/ Regimen | Type of Evidence | Key Findings | References |
| Chlorcyclizine ± Ribavirin | Antihistamine | Chronic HCV infection (adjunct) | Inhibits late‑stage viral entry | CCZ 75 mg bid ± RBV 1000/1200 mg/day | Randomized proof‑of‑concept | No sustained effect with CCZ alone; >3‑fold RNA reduction in 58% with CCZ+RBV | [63] |
| Meclizine | Antihistamine/ antiemetic | Achondroplasia (bone growth) | FGFR3 signaling inhibition in chondrocytes | 12.5–25 mg/day × 14 days (children) | Phase 1b | Well tolerated; achieved steady‑state plasma; supportive of growth therapy potential | [66] |
| Fexofenadine + Ramipril | Antihistamine + ACE inhibitor | Diabetic kidney disease | Anti‑inflammatory/ antioxidant; renal protection | Fexofenadine 60 mg/day (with ramipril) | Randomized clinical trial | ↓ albuminuria (UACR −16%); preserved eGFR; ↓ MCP‑1, 8‑OHdG, PCX | [67] |
HCV: Hepatitis C Virus | CCZ: Chlorcyclizine | RBV: Ribavirin | FGFR3: Fibroblast Growth Factor Receptor 3 | ACH: Achondroplasia | UACR: Urinary Albumin-to-Creatinine Ratio | eGFR: Estimated Glomerular Filtration Rate | MCP-1: Monocyte Chemoattractant Protein-1 | 8-OHdG: 8-Hydroxy-2′-Deoxyguanosine | PCX: Podocalyxin
Limitations of the Review
This review is subject to several limitations, including potential publication bias favoring positive findings, heterogeneity in study designs, dosing regimens, and outcome measures, which complicate direct comparisons across studies. Additionally, many included reports are based on preclinical models or small-scale clinical trials, limiting generalizability. The absence of standardized protocols and incomplete reporting of adverse effects further restricts the ability to draw definitive conclusions. Future systematic reviews and meta-analyses with rigorous inclusion criteria are needed to validate these findings and minimize bias.
CONCLUSION
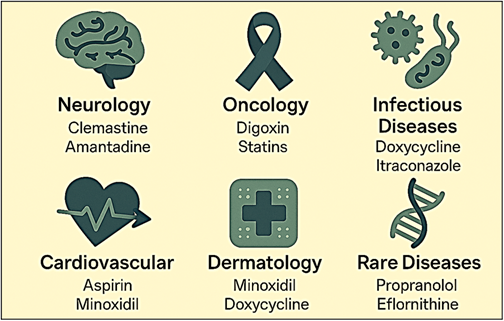
Drug repurposing provides a rapid, cost-effective pathway for discovering new treatments across multiple disease areas. Notable examples include clemastine and amantadine for neurological disorders, digoxin, statins, and aspirin for various cancers, minoxidil for hair loss, and propranolol for infantile hemangioma (Figure II). These cases highlight the ability of existing drugs to exert novel therapeutic effects through diverse mechanisms. However, translating preclinical and early clinical findings into approved therapies remains challenging due to limitations in assay validity, model relevance, trial design, and disease complexity. Future strategies should emphasize rigorous clinical validation through large, randomized trials, mechanistic and translational research to confirm drug behavior in humans, and target repurposing using genomics and AI to identify responsive subgroups. Additional priorities include exploring combination therapies, developing advanced delivery systems, addressing regulatory and intellectual property barriers, and ensuring long-term safety monitoring. Therapeutic areas with the greatest repurposing potential include neurology, oncology, cardiovascular disorders, dermatology, and rare diseases, where unmet clinical needs and shared biological pathways create opportunities for innovative treatment approaches. By focusing on these areas, drug repurposing can accelerate treatment development and improve patient outcomes across a broad spectrum of conditions (Figure III).
ACKNOWLEDGEMENT
The authors disclose utilizing Microsoft’s Copilot AI technology for assistant on Figure II and Figure III and language editing
CONFLICT OF INTEREST
The authors have no conflict of interest to report. REFERENCE
REFERENCE
- Rapicavoli RV, Alaimo S, Ferro A, Pulvirenti A. Computational methods for drug repurposing. Adv Exp Med Biol 2022; 1361: 119-141. https://doi.org/10.1007/978-3-030-91836-1_7
- Hodos RA, Kidd BA, Shameer K, Readhead BP, Dudley JT. In silico methods for drug repurposing and pharmacology. Wiley Interdiscip Rev Syst Biol Med 2016; 8(3): 186-210. https://doi.org/10.1002/wsbm.1337
- Hayes CD, Dey D, Palavicini JP, Wang H, Patkar KA, Minond D, et al. Striking reduction of amyloid plaque burden in an Alzheimer’s mouse model after chronic administration of carmustine. BMC Med 2013; 11(1): 81. https://doi.org/10.1186/1741-7015-11-81
- Wilkinson GF, Pritchard K. In vitro screening for drug repositioning. J Biomol Screen 2015; 20(2): 167-179. https://doi.org/10.1177/1087057114563024
- Halatsch ME, Dwucet A, Schmidt CJ, Mühlnickel J, Heiland T, Zeiler K, et al. In vitro and clinical compassionate use experiences with the drug-repurposing approach CUSP9v3 in glioblastoma. Pharmaceuticals (Basel) 2021; 14(12): 1241. https://doi.org/10.3390/ph14121241
- Amantea D, Certo M, Bagetta G. Drug repurposing and beyond: the fundamental role of pharmacology. Funct Neurol 2015; 30(1): 79. https://doi.org/10.11138/fneur/2015.30.1.079
- Chang HWK, Chang VHS. Animal models and in vivo investigations for drug repurposing in lung cancer. In: Drug Repurposing in Cancer Therapy: Approaches and Applications. Elsevier 2020: 273-293. https://doi.org/10.1016/B978-0-12-819668-7.00010-5
- Chakraborty C, Sharma AR, Bhattacharya M, Agoramoorthy G, Lee SS. The drug repurposing for COVID-19 clinical trials provide very effective therapeutic combinations: lessons learned from major clinical studies. Front Pharmacol 2021; 12: 704205. https://doi.org/10.3389/fphar.2021.704205
- Pahwa R, Tanner CM, Hauser RA, Sethi K, Isaacson S, Truong D, et al. Amantadine extended release for levodopa-induced dyskinesia in Parkinson’s disease (EASED Study). Mov Disord 2015; 30(6): 788-795. https://doi.org/10.1002/mds.26159
- Oertel W, Eggert K, Pahwa R, Tanner CM, Hauser RA, Trenkwalder C, et al. Randomized, placebo-controlled trial of ADS-5102 (amantadine) extended-release capsules for levodopa-induced dyskinesia in Parkinson’s disease (EASE LID 3). Mov Disord 2017; 32(12): 1701-1709. https://doi.org/10.1002/mds.27131
- Khlebtovsky A, Steiner I, Treves TA, Djaldetti R. Effect of repeated intravenous amantadine infusions in patients with Parkinson’s disease: an open-label pilot study. Clin Transl Sci 2019; 12(6): 586-590. https://doi.org/10.1111/cts.12684
- Espay AJ, Ostrem JL, Formella AE, Tanner CM. Extended-release amantadine for OFF-related dystonia in Parkinson’s disease. Parkinsonism Relat Disord 2024; 122: 106088. https://doi.org/10.1016/j.parkreldis.2024.106088
- Xing W, Huang P, Lu Y, Zeng W, Zuo Z. Amantadine attenuates sepsis-induced cognitive dysfunction possibly not through inhibiting toll-like receptor 2. J Mol Med (Berl) 2018; 96(5): 391-402. https://doi.org/10.1007/s00109-018-1631-z
- Yang S, Yu B, Zhang Q, Zhang Y, Fu L, Zhou B, et al. Amantadine modulates novel macrophage phenotypes to enhance neural repair following spinal cord injury. J Transl Med 2025; 23(1): 60. https://doi.org/10.1186/s12967-024-05916-y
- Delans K, Kelly K, Feldman SR. Treatment strategies, including antibiotics, to target the immune component of rosacea. Expert Rev Clin Immunol 2022; 18(12): 1239-1251. https://doi.org/10.1080/1744666X.2022.2128334
- Xiao W, Chen M, Wang B, Huang Y, Zhao Z, Deng Z, et al. Efficacy and safety of antibiotic agents in the treatment of rosacea: a systemic network meta-analysis. Front Pharmacol 2023; 14: 1169916. https://doi.org/10.3389/fphar.2023.1169916
- Normansell R, Sayer B, Waterson S, Dennett EJ, Del Forno M, Dunleavy A. Antibiotics for exacerbations of asthma. Cochrane Database Syst Rev 2018; 6: CD002741. https://doi.org/10.1002/14651858.CD002741.pub2
- Wang X, Shi H, Li X, Feng Y. Macrophages in rosacea: pathogenesis and therapeutic potential. Front Immunol 2025; 16: 1595493. https://doi.org/10.3389/fimmu.2025.1595493
- Chan SM, Tseng CL, Huang WH, Lin CT. Therapeutic assessment of diverse doxycycline-based formulations in promoting deep corneal wound healing: evidence from a rat model. Vet Sci 2025; 12(2): 143. https://doi.org/10.3390/vetsci12020143
- Di Nardo A, Holmes AD, Muto Y, Huang EY, Preston N, Winkelman WJ, et al. Improved clinical outcome and biomarkers in adults with papulopustular rosacea treated with doxycycline modified-release capsules in a randomized trial. J Am Acad Dermatol 2016; 74(6): 1086-1092. https://doi.org/10.1016/j.jaad.2016.01.023
- Ghimire JJ, Jat KR, Sankar J, Lodha R, Iyer VK, Gautam H, et al. Azithromycin for poorly controlled asthma in children: a randomized controlled trial. Chest 2022; 161(6): 1456-1464. https://doi.org/10.1016/j.chest.2022.02.025
- Chavez-Valdez R. Repurposing azithromycin for neuroprotection in neonates. Pediatr Res 2019; 86(4): 423-424. https://doi.org/10.1038/s41390-019-0443-3
- Lu C, Cheng D, Xie Y, Shang M, Chen R, Zhu Y, et al. Effect of CYP3A4 inhibitor and induction on the pharmacokinetics and safety of FHND9041, a novel EGFR T790M inhibitor, in healthy Chinese. BMC Pharmacol Toxicol 2025; 26(1): 97. https://doi.org/10.1186/s40360-025-00930-2
- Gerber DE, Putnam WC, Fattah FJ, Kernstine KH, Brekken RA, Pedrosa I, et al. Concentration-dependent early antivascular and antitumor effects of itraconazole in non-small cell lung cancer. Clin Cancer Res 2020; 26(22): 6017-6027. https://doi.org/10.1158/1078-0432.CCR-20-1916
- Farid N, Bux K, Ali K, Bashir A, Tahir R. Repurposing amphotericin B: antimicrobial, molecular docking and molecular dynamics simulation studies suggest inhibition potential of amphotericin B against MRSA. BMC Chem 2023; 17(1): 67. https://doi.org/10.1186/s13065-023-00980-9
- Machado PRL, Rosa MEA, Guimarães LH, Prates FVO, Queiroz A, Schriefer A, et al. Treatment of disseminated leishmaniasis with liposomal amphotericin B. Clin Infect Dis 2015; 61(6): 945-949. https://doi.org/10.1093/cid/civ416
- Pivonello R, Elenkova A, Fleseriu M, Feelders RA, Witek P, Greenman Y, et al. Levoketoconazole in the treatment of patients with Cushing’s syndrome and diabetes mellitus: results from the SONICS phase 3 study. Front Endocrinol (Lausanne) 2021; 12: 595894. https://doi.org/10.3389/fendo.2021.595894
- Fleseriu M, Pivonello R, Elenkova A, Salvatori R, Auchus RJ, Feelders RA, et al. Efficacy and safety of levoketoconazole in the treatment of endogenous Cushing’s syndrome (SONICS): a phase 3, multicentre, open-label, single-arm trial. Lancet Diabetes Endocrinol 2019; 7(11): 855-865. https://doi.org/10.1016/S2213-8587(19)30313-4
- Toodle V, Lee MH, Bachani M, Ruffin A, Vivekanandhan S, Malik N, et al. Fluconazole is neuroprotective via interactions with the IGF-1 receptor. Neurotherapeutics 2022; 19(4): 1313-1328. https://doi.org/10.1007/s13311-022-01265-0
- Parthsarathy V, Hölscher C. Chronic treatment with the GLP1 analogue liraglutide increases cell proliferation and differentiation into neurons in an AD mouse model. PLoS One 2013; 8(3): e58784. https://doi.org/10.1371/journal.pone.0058784
- Xie Y, Zheng J, Li S, Li H, Zhou Y, Zheng W, et al. GLP-1 improves the neuronal supportive ability of astrocytes in Alzheimer’s disease by regulating mitochondrial dysfunction via the cAMP/PKA pathway. Biochem Pharmacol 2021; 188: 114578. https://doi.org/10.1016/j.bcp.2021.114578
- Siddiqui N, Ali J, Parvez S, Zameer S, Najmi AK, Akhtar M. Linagliptin, a DPP-4 inhibitor, ameliorates Aβ (1-42) peptides induced neurodegeneration and brain insulin resistance (BIR) via insulin receptor substrate-1 (IRS-1) in rat model of Alzheimer’s disease. Neuropharmacology 2021; 195: 108662. https://doi.org/10.1016/j.neuropharm.2021.108662
- Kosaraju J, Holsinger RMD, Guo L, Tam KY. Linagliptin, a dipeptidyl peptidase-4 inhibitor, mitigates cognitive deficits and pathology in the 3xTg-AD mouse model of Alzheimer’s disease. Mol Neurobiol 2017; 54(8): 6074-6084. https://doi.org/10.1007/s12035-016-0125-7
- Fernandez-Martos CM, Atkinson RAK, Chuah MI, King AE, Vickers JC. Combination treatment with leptin and pioglitazone in a mouse model of Alzheimer’s disease. Alzheimers Dement (N Y) 2017; 3(1): 92-106. https://doi.org/10.1016/j.trci.2016.11.002
- Burns DK, Alexander RC, Welsh-Bohmer KA, Culp M, Chiang C, O’Neil J, et al. Safety and efficacy of pioglitazone for the delay of cognitive impairment in people at risk of Alzheimer’s disease (TOMMORROW): a prognostic biomarker study and a phase 3, randomised, double-blind, placebo-controlled trial. Lancet Neurol 2021; 20(7): 537-547. https://doi.org/10.1016/S1474-4422(21)00043-0
- Beheshti F, Hosseini M, Bakhtiari-Dovvombaygi H, Salmani H, Ahmadabady S, Marefati N, et al. Rosiglitazone attenuates amyloid beta and glial fibrillary acidic protein in the hippocampus and neuroinflammation associated learning and memory impairments in rats. Behav Brain Res 2023; 452: 114549. https://doi.org/10.1016/j.bbr.2023.114549
- Low S, Goh KS, Ng TP, Moh A, Ang SF, Wang J, et al. Association between use of sodium-glucose co-transporter-2 (SGLT2) inhibitors and cognitive function in a longitudinal study of patients with type 2 diabetes. J Alzheimers Dis 2022; 87(2): 635-642. https://doi.org/10.3233/JAD-215678
- Yue FG, Dong L, Hu TT, Qu XY. Efficacy of dapoxetine for the treatment of premature ejaculation: a meta-analysis of randomized clinical trials on intravaginal ejaculatory latency time, patient-reported outcomes, and adverse events. Urology 2015; 85(4): 856-861. https://doi.org/10.1016/j.urology.2015.01.009
- Abu El-Hamd M, Abdelhamed A. Comparison of the clinical efficacy and safety of the on-demand use of paroxetine, dapoxetine, sildenafil and combined dapoxetine with sildenafil in treatment of patients with premature ejaculation: a randomised placebo-controlled clinical trial. Andrologia 2018; 50(1): e12829. https://doi.org/10.1111/and.12829
- Zhang Y, Liu WQ, Hosseinpour Z, Pike GB, Cerchiaro G, Greenfield J, et al. Feasibility study to assess lesion repair in relapsing-remitting multiple sclerosis: a randomized controlled pilot clinical trial of domperidone add-on treatment. Mult Scler Relat Disord 2024; 85: 105525. https://doi.org/10.1016/j.msard.2024.105525
- Biederman J, Fried R, Tarko L, Surman C, Spencer T, Pope A, et al. Memantine in the treatment of executive function deficits in adults with ADHD: a pilot-randomized double-blind controlled clinical trial. J Atten Disord 2017; 21(4): 343-352. https://doi.org/10.1177/1087054714538656
- Kantor D, Panchal S, Patel V, Bucior I, Rauck R. Treatment of postherpetic neuralgia with gastroretentive gabapentin: interaction of patient demographics, disease characteristics, and efficacy outcomes. J Pain 2015; 16(12): 1300-1311. https://doi.org/10.1016/j.jpain.2015.08.016
- Brown S, Johnston B, Amaria K, Watkins J, Campbell F, Pehora C, et al. A randomized controlled trial of amitriptyline versus gabapentin for complex regional pain syndrome type I and neuropathic pain in children. Scand J Pain 2016; 13: 156-163. https://doi.org/10.1016/j.sjpain.2016.05.039
- Majdinasab N, Kaveyani H, Azizi M. A comparative double-blind randomized study on the effectiveness of duloxetine and gabapentin on painful diabetic peripheral polyneuropathy. Drug Des Devel Ther 2019; 13: 1985-1992. https://doi.org/10.2147/DDDT.S185995
- Hwang CJ, Lee JH, Kim JH, Min SH, Park KW, Seo HY, et al. Gabapentin versus transdermal fentanyl matrix for the alleviation of chronic neuropathic pain of radicular origin: a randomized blind multicentered parallel-group noninferiority trial. Pain Res Manag 2019; 2019: 4905013. https://doi.org/10.1155/2019/4905013
- Hwang K, Kim J, Kang SG, Jung TY, Kim JH, Kim SH, et al. Levetiracetam as a sensitizer of concurrent chemoradiotherapy in newly diagnosed glioblastoma: an open-label phase 2 study. Cancer Med 2022; 11(2): 371-379. https://doi.org/10.1002/cam4.4454
- Caponigro F, Di Gennaro E, Ionna F, Longo F, Aversa C, Pavone E, et al. Phase II clinical study of valproic acid plus cisplatin and cetuximab in recurrent and/or metastatic squamous cell carcinoma of head and neck: V-CHANCE trial. BMC Cancer 2016; 16(1): 918. https://doi.org/10.1186/s12885-016-2957-y
- Ibrahim SM, Kamel AS, Ahmed KA, Mohammed RA, Essam RM. The preferential effect of clemastine on F3/contactin-1/Notch-1 compared to Jagged-1/Notch-1 justifies its remyelinating effect in an experimental model of multiple sclerosis in rats. Int Immunopharmacol 2024; 128: 111481. https://doi.org/10.1016/j.intimp.2023.111481
- Kawakami S, Nagasawa Y, Hagiwara-Nagasawa M, Omura K, Aimoto M, Takahara A. Torsadogenic potential of a novel remyelinating drug clemastine for multiple sclerosis assessed in the rabbit proarrhythmia model. J Pharmacol Sci 2020; 144(3): 123-128. https://doi.org/10.1016/j.jphs.2020.08.003
- Zhang X, Shi X, Zhang X, Zhang Y, Yu S, Zhang Y, et al. Repositioning fluphenazine as a cuproptosis-dependent anti-breast cancer drug candidate based on TCGA database. Biomed Pharmacother 2024; 178: 117293. https://doi.org/10.1016/j.biopha.2024.117293
- Chu DK, Freitag T, Marrin A, Walker TD, Avilla E, Freitag A, et al. Peanut oral immunotherapy with or without H1 and H2 antihistamine premedication for peanut allergy (PISCES): a placebo-controlled randomized clinical trial. J Allergy Clin Immunol Pract 2022; 10(9): 2386-2394. https://doi.org/10.1016/j.jaip.2022.05.015
- Klöcker N, Hanschke W, Toussaint S, Verse T. Scopolamine nasal spray in motion sickness: a randomised, controlled, and crossover study for the comparison of two scopolamine nasal sprays with oral dimenhydrinate and placebo. Eur J Pharm Sci 2001; 13(2): 227-232. https://doi.org/10.1016/S0928-0987(01)00107-5
- Khorana M, Wongsin P, Torbunsupachai R, Kanjanapattanakul W. Effect of domperidone on breast milk production in mothers of sick neonates: a randomized, double-blinded, placebo-controlled trial. Breastfeed Med 2021; 16(3): 245-250. https://doi.org/10.1089/bfm.2020.0234
- Jyothi B, Mitragotri MV, Kurugodiyavar MD, Shaikh SI, Korikanthimath VV. Morphine versus loperamide with Intrasite gel in the treatment of painful dermal ulcers: a randomized, crossover study. Pain Physician 2021; 24(1): E37-E44. https://doi.org/10.36076/ppj.2021.24.E37-E44
- De Lisle RC, Mueller R, Roach E. Lubiprostone ameliorates the cystic fibrosis mouse intestinal phenotype. BMC Gastroenterol 2010; 10(1): 107. https://doi.org/10.1186/1471-230X-10-107
- Betari N, Sahlholm K, Morató X, Godoy-Marín H, Jáuregui O, Teigen K, et al. Inhibition of tryptophan hydroxylases and monoamine oxidase-A by the proton pump inhibitor omeprazole: in vitro and in vivo investigations. Front Pharmacol 2020; 11: 593416. https://doi.org/10.3389/fphar.2020.593416
- Li L, Hu M, Wang T, Chen H, Xu L. Repositioning aspirin to treat lung and breast cancers and overcome acquired resistance to targeted therapy. Front Oncol 2019; 9: 1503. https://doi.org/10.3389/fonc.2019.01503
- Wang Y, Ma Q, Zhang S, Liu H, Zhao B, Du B, et al. Digoxin enhances the anticancer effect on non-small cell lung cancer while reducing the cardiotoxicity of adriamycin. Front Pharmacol 2020; 11: 186. https://doi.org/10.3389/fphar.2020.00186
- Sanabria BD, Perdomo YC, Miot HA, Ramos PM. Oral minoxidil 7.5 mg for hair loss increases heart rate with no change in blood pressure in 24 h Holter and 24 h ambulatory blood pressure monitoring. An Bras Dermatol 2024; 99(5): 734-736. https://doi.org/10.1016/j.abd.2023.08.016
- Léauté-Labrèze C, Hoeger P, Mazereeuw-Hautier J, Guibaud L, Baselga E, Posiunas G, et al. A randomized, controlled trial of oral propranolol in infantile hemangioma. N Engl J Med 2015; 372(8): 735-746. https://doi.org/10.1056/NEJMoa1404710
- Wang KH, Liu CH, Ding DC. Statins as repurposed drugs in gynecological cancer: a review. Int J Mol Sci 2022; 23(22): 13937. https://doi.org/10.3390/ijms232213937
- Jiang W, Hu JW, He XR, Jin WL, He XY. Statins: a repurposed drug to fight cancer. J Exp Clin Cancer Res 2021; 40(1): 241. https://doi.org/10.1186/s13046-021-02041-2
- Hamdan M, Kulabaş N, Küçükgüzel İ. In silico evaluation of H1-antihistamines as potential inhibitors of SARS-CoV-2 RNA-dependent RNA polymerase: repurposing study of COVID-19 therapy. Turk J Pharm Sci 2025; 21(6): 566-576. https://doi.org/10.4274/tjps.galenos.2024.49768
- Glisic S, Stevanovic K, Perdih A, Bukreyeva N, Maruyama J, Perovic V, et al. Influenza A virus inhibition: evaluating computationally identified cyproheptadine through in vitro assessment. Int J Mol Sci 2025; 26(13): 5962. https://doi.org/10.3390/ijms26135962
- Koh C, Dubey P, Han MAT, Walter PJ, Garraffo HM, Surana P, et al. A randomized, proof-of-concept clinical trial on repurposing chlorcyclizine for the treatment of chronic hepatitis C. Antiviral Res 2019; 163: 149-155. https://doi.org/10.1016/j.antiviral.2019.01.017
- Matsushita M, Kitoh H, Mishima K, Kamiya Y, Kato D, Takemoto G, et al. Phase 1b study on the repurposing of meclizine hydrochloride for children with achondroplasia. PLoS One 2023; 18(7): e0283425. https://doi.org/10.1371/journal.pone.0283425
- El-Fatatry BM, El-Haggar SM, Ibrahim OM, Shalaby KH. Repurposing fexofenadine as a promising candidate for diabetic kidney disease: randomized clinical trial. Int Urol Nephrol 2024; 56(4): 1395-1402. https://doi.org/10.1007/s11255-023-03804-w
Please cite this article as:
Farag M. Azab, Mohammed H. Abo-Mandour, Mostafa M. Hassanein, Mariam A. Khidr, Yousef M. Al-Taher and Mona F. Mahmoud, Drug Repurposing and Its Potential Roles in Drug Discovery. Malaysian Journal of Pharmacy (MJP). 2026;1(12):5-21. https://mjpharm.org/drug-repurposing-and-its-potential-roles-in-drug-discovery/