ABSTRACT
Introduction: Poor medication adherence has been a major problem leading to suboptimal treatment outcomes. Existing studies suggest that telehealth interventions may improve medication adherence among patients. In Malaysia, there is a paucity of published studies on the impact of telehealth on medication adherence. Objective: This study aimed to evaluate the effect of telehealth on medication adherence among hypertensive patients with suboptimal medication adherence. Methods: Patients who met the inclusion criteria, with a Medication Possession Ratio (MPR) of less than 80 (n=60), were recruited via convenience sampling and randomized into a control (n=30) and an intervention group (n=30) using a random permuted blocks technique. This randomization list was accessible only to the principal investigator. Individualized medication charts, reading materials, and medication adherence reminders were sent via Whatsapp to patients in the intervention group weekly. Patients from both groups were followed up for 12 weeks, with prescription refills provided at weeks 4 and 12. Patients’ medication adherence, measured by MPR and pill count (PC), were recorded. Results: Overall, there was a statistically significant improvement in adherence measured using MPR for patients in both control (p<0.01) and intervention groups (p<0.01). However, adherence measured using PC at weeks 4 and 12 did not show any significant improvement in either group. When comparing medication adherence between the control and intervention groups, patients in the intervention group demonstrated significantly better improvement compared to those in the control group for both methods: MPR (p<0.01) and PC (p<0.05). Conclusion: Telehealth interventions delivered through informative and reminder text messages demonstrated significantly higher level of medication adherence.
INTRODUCTION
Poor medication adherence has always been a major concern and is recognized as a significant and persistent challenge in our healthcare system ever since its establishment. In 2013, the World Health Organization (WHO) reported that approximately half of the patients with chronic illnesses do not comply with their prescribed medication [1]. Past studies have shown that the non-adherence rate in Malaysia ranges from 46.6% to 56% [2,3,4]. Poor medication adherence leads to unfavourable patient outcomes as well as increased medical expenditure. In the United States America, non-adherence to treatment itself leads to an additional $100 – 300 billion in healthcare costs [5, 6]. In Malaysia, various initiatives including the establishment of the Medication Therapy Adherence Clinic (MTAC) has been implemented over the years to improve patient adherence. However, adherence to MTAC follow-ups and timely prescription refills became increasingly challenging during the coronavirus (COVID-19) pandemic.
Although COVID-19 created heightened challenges, particularly in adherence, telehealth services gained popularity as a tool to improve patients’ adherence. Over the years, telehealth has been extensively studied, and several benefits have been demonstrated, including improved patient care, enhanced accessibility, better medication adherence, and reduced costs [7]. A systematic review, conducted through searches of five databases, highlighted the role of telehealth during the COVID-19 outbreak in the prevention, diagnosis, management, and treatment of COVID-19. During the pandemic, telehealth conducted via the internet, telephone consultations, social media messaging, and live video conferencing showed impactful outcomes in preventing morbidity and reducing patient presence in high-risk public areas [8].
Malaysia’s age-old Telemedicine Blueprint was established by the Ministry of Health on 25 July 1997. The coronavirus pandemic acted as a catalyst to improve Malaysia’s telehealth industry, which had failed to gain mainstream adoption over the years. In Malaysia, DoctorOnCall offers teleconsultation, medication delivery, and Covid-19 screening services, whereas HomeGP connects patients with house-call doctors and trained home care nurses.
Numerous studies have specifically examined the use of telehealth as a tool to improve patient medication adherence. Research on the effects of telehealth interventions on medication adherence among patients with diabetes, hypertension, and dyslipidaemia has shown that telehealth modalities, including telephonic outreach and specialized tools designed to increase health literacy, have been associated with improved Medication Possession Ratio (MPR) and Proportion of Days Covered (PDC) rates. Other studies involving telehealth and medication adherence in transplant patients showed reduced mean tacrolimus standard deviation; asthma patients showed higher satisfaction, and antiretroviral treatment demonstrated increased adherence [9]. In Malaysia, a study using automated short message service to improve medication adherence following acute coronary syndrome also showed higher medication adherence in the intervention group [10]. Conversely, a study by Olliver et al. (2009) showed reduced adherence in both the control and intervention groups despite daily text message (TM) reminders. In this study, 63% of participants agreed that the reminders were not annoying [11].
From studies examining the use of telehealth to assess medication adherence, it is important to note that the tools and strategies used varied across each study. Telehealth strategies included the use of TMs with requests to acknowledge receipt after taking pills, TM reminders plus health information, side effects information [9], Real Time Medication (RTM) monitoring combined with TMs [12], mobile apps (e.g., Pillbox reminder), and telephone calls. These strategies are consistent with the WHO multidimensional adherence model, which posits that there is no single determinant responsible for non-adherence to treatment. Adherence is multidimensional phenomenon influenced by patient-related factors, socioeconomic factors, healthcare system-related factors, condition-related factors, and treatment-related factors. Adherence interventions aimed at improving adherence should be tailored to address and identify patients’ fundamental reasons for non-adherence [10].
Outcome measures in telehealth-related studies on medication adherence also vary across studies, which complicates the generalization of findings. Some studies utilize self-reporting methods, while others employ pill counts method. More accurate methods include measuring serum concentrations of the studied medication. Each method has its advantages and disadvantages. Some studies were designed with controls; however, baseline adherence to medication was never recorded. A recent study published in Malaysia by Xiaoye Li et al. (2022), comparing pharmacist-led telemedicine intervention and a controlled group, used numerical blood pressure measurement as a tool to evaluate adherence and blood pressure [13].
The types of non-adherence and factors affecting them may differ between countries. The types of reported non-adherence, as reviewed by Jin J. et al. (2008), include: receiving a prescription but not filling it, taking an incorrect dose, taking medications at the wrong times, increasing or decreasing the frequency of doses, stopping treatment too soon, delays in seeking healthcare, non-participation in clinic visits, failure to follow doctor’s instructions, drug holidays, and “white coat” adherence [14]. Furthermore, intentional and unintentional non-adherence to medication is considered a patient-related factor [15].
Malaysia is a multi-ethnic, multicultural, and multilingual nation that operates under two types of healthcare systems: government and co-existing private healthcare settings [16]. Studies and telehealth tools designed to improve medication adherence in Malaysia should be unique to its patient population and healthcare setting. For example, real-time medication monitoring (RTMM) is not available in Malaysia; hence, such studies are not applicable in our healthcare setting. Mobile apps such as Pillbox reminder are only available in English, which may be challenging for many of our patients. Many studies also focus on the primary types of non-adherence which concluded that the cost of medication could be a reason patients do not fill their prescriptions. In Malaysia, public healthcare medications are free and readily available to all patients.
There are only a few studies available in Malaysia measuring the effects of telehealth on medication adherence. Additionally, studies conducted in the last decade may not be applicable due to advancements in technology and new communication applications. Now, more elderly individuals are technology-savvy compared to the past. Available studies of telehealth in Malaysia previously used self-reporting questionnaire (e.g., Morisky scale) as their outcome measure, which is highly susceptible to bias [9]. Thus, this study was conducted to measure the outcome of telehealth using the MPR method and pill count (PC) method as our main tools of measurement.
Our aim was to evaluate the effects of telehealth in the form of educative and reminder text message (TMs) on medication adherence to oral medications in patients with hypertension who have a suboptimal level of adherence, using both the MPR method and the PC method.
METHOD
Study design
This pilot study collected data at weeks 0, 4, and 12. At week 0, all recruited participants had their prescriptions filled up with a 28-day supply of tablets. All medication blisters given to participants were marked “R” in red, and they were advised to consume only the medications from the marked blisters throughout the 4 weeks. They were instructed to keep all empty blisters for review at the next follow-up at week 4. All participants received standard medications over the dispensing counter.
Participants were then randomized to either a control group or an intervention Text Message (TM) group. At week 4, participants returned all the marked blisters to the designated pharmacist and were subsequently given an additional 8-week supply of medication. They were instructed to bring back all the marked blisters at week 12 for assessment of medication adherence.
The medication adherence rate was evaluated via the Medication Possession Ratio (MPR) and pill count (PC) method. For the intervention group, participants received TM reminders and could respond accordingly. All participants were informed of the aim of the study. The primary outcome measure of the study was the rate of medication adherence.
Study population
The study participants receiving antihypertensive medications who obtained their medications from the outpatient pharmacy of Hospital Bukit Mertajam, with suboptimal adherence (MPR<80%) in their previous prescriptions, were selected via convenience sampling. In accordance with Haynes’s early empirical definition, adequate adherence to antihypertensive medications was defined as taking ≥80% of the prescribed doses[17]. Informed consent was obtained from the patients after they had reviewed the patient information leaflet thoroughly.
Inclusion criteria
1) Adults > 18 years old
2) Diagnosis of hypertension on at least ONE antihypertensive medication under outpatient follow-up
3) Medication list consists of only tablets formulations
4) Prescriptions with at least 3 months remaining validity
5) Participants with MPR < 80%
Exclusion criteria
1) Multiple follow-ups/ multiple prescriptions
2) Patients or caregivers who serve medication did use WhatsApp messenger
3) Patients whose medication regime was expected to be frequently altered (e.g., dialysis patients)
4) Current active MTAC patients
5) Patients who had leftover medication at home prior to enrolment
6) Patient who are unable to follow the study protocol
Sample size
In a previous study, the responses within each subject group were normally distributed with a standard deviation of 19.5 [18]. If the true difference in the experimental and control means is 17.8, then 19 experimental subjects and 19 control subjects were required to reject the null hypothesis that the population means of the experimental and control groups are equal, with a probability (power) of 0.8. The Type I error probability associated with this test of the null hypothesis is 0.05. Anticipating a dropout rate of around 50%, the target sample size was rounded up to 30 participants for each study arm.
Randomization
In this study, the recruited participants were randomized via a random permuted blocks technique. A randomization list was pre-generated via Sealed Envelope Ltd. 2017[19]. Different lengths of blocks were used to blind the investigator of the possibility of the next allocation. This list was only accessible to the principal investigator. After receiving informed consent, investigators obtained the allocation for each participant. Participant data were locked within the randomization list and stored in a password-protected file, only accessible by the principal investigator.
To avoid any bias or fabrication of data, the personnel involved in the pill count process at the end of weeks 4 and 12 were blinded to participants’ group allocation and randomization.
Telehealth Tools and Design for Intervention group
A text-message-based telehealth program was designed for this study. Communication between potential subjects and pharmacists was carried out using “text messages” or “voice messages” via WhatsApp in subject’s preferred language (three languages: English, Bahasa Melayu, and Mandarin were offered). A smartphone (Samsung Galaxy) with the phone number “012abcdefg” was used to communicate with subjects. The contact and particular data of every selected subject were verified at week 0 via WhatsApp. Only subjects with verified particulars were selected to proceed in the study. Throughout the study period, telehealth service was provided to subjects via a series of standard questions. The standard text messages and reading materials in multiple language were validated by a senior healthcare professional proficient in the respective languages.
The text message-based telehealth designed for this study aimed to overcome both intentional and unintentional non-adherence. All messages were typed in one of the participants’ preferred languages. These messages encompassed four key elements as outlined below:
- Individual medication use chart
At week 0, a photo of the participant’s prescription was taken to prepare a chart specifically for each patient. The chart summarized each participant’s current medications, including drug identifications, doses, frequencies, indications, times of administration, and other special instructions for medications. Once prepared, the chart was counterchecked by a second pharmacist for accuracy. The finalized chart was then sent to participants via WhatsApp, and they were encouraged to use it as a guide for their medication use.
- Reading materials to improve adherence to medicines
Reading materials were sent to subjects on weeks 1, 2, 3, 4, 5, 7, 9, and 11. The topics included:
Week 1 – “Definition of Medication Adherence”
Week 2 – “Impact of Medication Non-adherence I”
Week 3 – “Impact of Medication Non-adherence II”
Week 4 – “ How do I remember to take medicines?”
Week 5 – “BP Target and Measuring Technique”
Week 7 – “What happens if I forget to take antihypertensive medicines?”
Week 9 – “Complications of Uncontrolled Hypertension” Week 11 – “Non-pharmacological management of Hypertension”
All materials were prepared by pharmacists at Hospital Bukit Mertajam.
- Reminder on adherence to medications
Pharmacists sent reminders about adherence to medications weekly on weeks 1, 2, 3, 4, 5, 7, 9 and 11 via WhatsApp. Subjects were encouraged to communicate with pharmacists regarding their adherence status.
- Addressing the subject’s medical concerns
This was a personalized, interactive text messaging service provided via telehealth. Pharmacists addressed the subjects’ medical concerns from weeks 0 to week 11 with the utmost goal of improving adherence and safe use of medications.
Medication possession ratio (MPR), pill count (PC), and medication adherence rate
All marked tablet blisters returned at weeks 4 and 12 were collected and calculated. The medication adherence rate of patients in this study was measured using two methods: Medication Possession Ratio (MPR) and pill count (PC) method. These assessment tools were selected due to their low cost and less susceptible to reporting biases.
MPR was calculated at baseline (week 0), at week 4, and at week 12 using the following formula [20]:
Changes in MPR were analyzed within each group, and differences in MPR between the treatment and control groups were also compared.
The pill count rate was calculated using the following formula [21]:
Pill count rates for both groups at weeks 4 and 12 were then tabulated for comparison between the intervention and control groups. Any changes in medication adherence rates over time between both groups were also compared.
Study duration and timeline
Stage 1: Review of different literatures and journals – 2 months
Stage 2: Protocol preparation, presentation, and submission – 2
months
Stage 3: Text message material preparation and validation – 1
months
Stage 4: Data collection and data analysis – 6 months
Stage 5: Result write-up and presentation – 3 months
Risks and benefits to study participants
This pilot study was safe, with no serious adverse outcomes observed. All recruited patients received standard dispensing of all prescribed medications. Additional text messages were sent to the intervention groups. This study may help demonstrate whether the use of TM could potentially improve patient’s adherence to medication without face-to-face counselling.
The study received ethical approval from the Medical Review and Ethics Committee, Ministry of Health, Malaysia. The registration ID for the National Medical Research Register is NMRR ID: NMRR-21-1882-60440.
RESULT
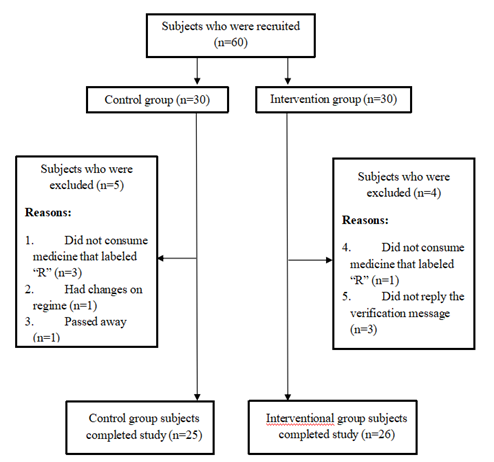
A total of 60 participants were recruited for this study and were randomized equally into both the control group (30 subjects) and the intervention group (30 subjects).
Nevertheless, due to the reasons stated in Figure Ⅰ, the final number of participants who enrolled and completed the study was 51. The socio-demographic data of the participants recruited for the study are presented in Table Ⅰ. There were no significant differences in gender, educational level, marital status, race, living arrangement, and employment between the control and intervention groups. The comparison of both the MPR and pill count between the control and intervention groups for weeks 5-12 and weeks 1-12 showed significant differences (p<0.05).
Table Ⅰ. Socio-demographic characteristic of study participants randomized to receive either telehealth text message or standard over-the-counter dispensing.
| Characteristics | Overall (n=51) | Control group (n=25) | Intervention group (n=26) | p-value |
| Median Age (Year; Range) | 62 (55-71) | 64 (55.5-71) | 61 (54-69) | 0.559a |
| Gender | ||||
| Male | 25 | 12 | 13 | 0.886b |
| Female | 26 | 13 | 13 | |
| Educational level | ||||
| Unschooled | 6 | 5 | 1 | 0.07b |
| Primary | 16 | 10 | 6 | |
| Secondary | 25 | 10 | 15 | |
| Diploma | 2 | 0 | 2 | |
| Degree | 2 | 0 | 2 | |
| Marital status | ||||
| Married | 44 | 20 | 24 | 0.342b |
| Single | 2 | 1 | 1 | |
| Widower | 5 | 4 | 1 | |
| Race | ||||
| Malay | 13 | 5 | 8 | 0.639b |
| Chinese | 20 | 10 | 10 | |
| Indian | 18 | 10 | 8 | |
| Living arrangement | ||||
| Alone | 6 | 5 | 1 | 0.073b |
| With family | 45 | 20 | 25 | |
| Employment | ||||
| Yes | 22 | 10 | 12 | 0.657b |
| No | 29 | 15 | 14 |
p-value > 0.05 shows no significant difference; “a” generated via Mann Whitney Test; “b” generated via chi-square test.
The intervention group showed better adherence during weeks 5-12 and 1-12. For pre and post-comparison, both the control and intervention groups demonstrated significant improvement in MPR when
comparing baseline versus weeks 1-4, baseline versus weeks 5-12, and baseline versus weeks 1-12 (p<0.05), indicating that both groups showed improvement in adherence compared to baseline. However, the MPR between weeks 1-4 and weeks 5-12 did not show significant differences (p>0.05). Similarly, the pill count comparisons between weeks 1-4 and weeks 5-12 did not show significant differences (p>0.05).
DISCUSSION
At week 0, the MPR of control group was not significantly different from intervention group (p>0.05), reflecting similar baseline adherence between the two groups at the time of enrollment. During weeks 1-4, both groups manifested a similar trend of MPR improvement, resulting in no significant difference of MPR between the two groups (p>0.05). However, the MPR of the intervention group was significantly higher compared to the control group at weeks 5-12 and 1-12 (p<0.05).
Table Ⅱ. Study outcome results (MPR and Pill Count) by group.
| Parameter | Control (n=25) | Intervention (n=26) | p-value between group | ||
| Median (IQR) | p-value (within group) | Median (IQR) | p-value (within group) | ||
| MPR | |||||
| Baseline | 71.4 (59.2-76.6) | N/A | 71.4 (62.0-76.8) | N/A | 0.828 |
| Weeks 1-4 | 96.6(82.0-100) | N/A | 100 (87.7-100) | N/A | 0.26 |
| Weeks 5-12 | 90.3(76.3-97.4) | N/A | 100 (94.5-100) | N/A | <0.001 |
| Weeks 1-12 | 86.6(80.4-97.7) | N/A | 97.4 (91.0-100) | N/A | 0.002 |
| Baseline vs Weeks 1-4 | N/A | <0.001 | N/A | <0.001 | N/A |
| Baseline vs Weeks 5-12 | N/A | <0.001 | N/A | <0.001 | N/A |
| Baseline vs Weeks 1-12 | N/A | <0.001 | N/A | <0.001 | N/A |
| Weeks 1-4 vs Weeks 5-12 | N/A | 0.735 | N/A | 0.304 | N/A |
| Pill Count | |||||
| Weeks 1-4 | 88.1(71.8-100) | N/A | 95.9 (89.3-99.6) | N/A | 0.23 |
| Weeks 5-12 | 85.6(76.3-99.0) | N/A | 96.5 (89.5-100) | N/A | 0.044 |
| Weeks 1-12 | 87.0(75.75-95.9) | N/A | 95.1 (89-98.6) | N/A | 0.044 |
| Weeks 1-4 vs Weeks 5-12 | N/A | 0.911 | N/A | 0.761 | N/A |
p-value < 0.05 shows significant difference; generated via Mann Whitney Test (between group) and Wilcoxon signed-rank test (within group).
A similar trend was observed when using the pill count rate as a measure of adherence in this study.
This outcome corresponds with the findings of Li et al. (2022), which highlighted that pharmacist-led telemedicine could significantly improve medication adherence, especially during the COVID-19 pandemic, and lead to better blood pressure control in hypertension management [13]. Additionally, similar results were reported in other studies examining different medical conditions. For example, Sahar et al. (2014) concluded that an automated SMS-based reminder system potentially enhanced medication adherence in patients with acute coronary syndrome [10]. Furthermore, Strandbygaard et al. (2010) showed that sending daily text message reminders to asthma patients significantly increased adherence levels in the intervention group after 12 weeks [17]. Likewise, higher adherence to antiretroviral therapy was observed in participants who received SMS reminders, according to Pop et al. (2011) [22]. Among diabetic patients receiving intensive insulin therapy, a text-messaging support system was found to improve self-reported adherence, as noted by Franklin et al. (2006) [23].
The improvement in adherence observed in this study suggests that electronic text-based programs may enhance therapeutic outcomes. A systematic review found that patient reinforcement was the most promising category of interventions to improve adherence in cardiovascular disease, as indicated by Schedlbauer et al. (2010) [24]. Additionally, Van et al. (2012) categorized reminders as behavioural interventions for patients to take their medications [25]. Electronic text-based programs could serve as convenient tools to provide reinforcement and reminders for behavioural changes. Indeed, Cutrona et al. (2010) also reported electronic text-based programme as successful modes of intervention delivery to improve cardiovascular medication adherence [26]. The use of a reminder system, electronic materials on anti-hypertensive medication, together with Question-and-Answer service via an electronic text-based program in this pilot study, has proven effective in improving compliance. The outcomes of this pilot study are consistent with findings from previous studies. This study provides promising data to support the role of pharmacists in enhancing patient’s compliance with hypertension medications through a simple telehealth application, maximizing hypertension management. This is especially useful during pandemic periods, such as the COVID-19 pandemic, when healthcare workers are required to minimize face-to-face contact, as well as reduce time and costs, as shown in Li et al. (2022) and Bokolo et al. (2020) [13, 27].
In this study, changes in MPR and pill count were observed over time for both the control and intervention groups. From Table Ⅱ, the baseline MPR was 71.4 (60.7-76.6), and by week 4, the MPR value improved to 100 (82.4-100) (p < 0.001). We observed that the same phenomena were seen in control group at week 12 when comparing to the baseline MPR. The main reason for this improvement may be explained by the fact that the control group was aware that that they were enrolled in the study at the time of consent, as well as the marking of their medication blisters. Both of these factors likely contributed to the improvement in adherence to medicine regimen.
For the intervention group, the improvement in MPR from baseline to week 4 was statistically significant. The MPR improvement for week 12 compared to baseline was also statistically significant. This is in line with the findings of Xiaoye Li et al. (2022), which showed that pharmacist-conducted patient counselling is more likely to enhance medication adherence (19.1 vs. 7.3%, p= 0.001) [13]. However, similar results were observed in the control group during the same period. Hence, it will be challenging to determine whether these results were due to study consent and marked blisters or the telehealth intervention.
The MPR for weeks 5-12 was not statistically different compared to the MPR results from weeks 1-4. The MPR value was already 100 (87.73-100) at week 4, leaving limited room for improvement for patients. The positive results persisted until week 12, showing an MPR value of 100 (94.5-100). A similar pattern was observed when adherence was measured using pill count. By week 4, the pill count result was 95.9 (89.3-99.55), with similar results observed at week 12. Since the week 4 pill count does not represent the baseline pill count results, it is difficult to detect further improvement when comparing to week 12 pill count results. This suggests that adherence improvement might have start to take place from weeks 0 to 4.
The results of the pre-post comparison do not highlight the advantage of telehealth in this study, as both groups showed improvement from baseline. However, the effect of telehealth services can be seen when comparing both the control and intervention groups. The MPR and pill count were significantly better during weeks 5-12 and 1-12. Future studies should incorporate a longer follow-up duration, as extended observation periods may yield different outcomes in both intervention and control groups during long-term pre–post comparisons.
Limitations
Our study has several limitations. First, this study appears to be a single-centered study with a relatively small sample size. Furthermore, our study did not measure relationship between medication adherence and blood pressure control. Moreover, our data collection followed participants for a total of three months, which is a relatively short time frame. Thus, further studies with a larger sample size that involve other facilities and a longer follow-up time frame are needed to be carried out to support the findings of this study.
CONCLUSION
Telehealth interventions delivered through informative and reminder text messages demonstrated significantly higher medication adherence compared with the control group. In addition, both the intervention and control groups showed significant improvements in medication adherence relative to baseline.
ACKNOWLEDGEMENT
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. We would like to thank the Director General of Health Malaysia for his permission to publish this article. We are also very grateful to Gooi Jia Nian and Ling Jing Kai for assisting us during the data collection period. Furthermore, we would like to express our gratitude to Prashant A/L Subramanian, Noraniza Binti Ahamd, Suraniza Binti Suhaimi, Loh Hong Chuan, and Tan Yee Mun for their opinions and validation of the educational materials. Lastly, we would like to thank our facility, Hospital Bukit Mertajam, where the study was conducted.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCE
- World Health Organization. Adherence to long-term therapies: evidence for action. Geneva: World Health Organization; 2003. Available from: https://iris.who.int/handle/10665/42682
- Aziz AM, Ibrahim MI. Medication noncompliance: a thriving problem. Med J Malaysia. 1999; 54(2): 192–199. https://pubmed.ncbi.nlm.nih.gov/10972029/
- Turki AK, Sulaiman SAS. Elevated blood pressure among patients with hypertension in a general hospital of Penang, Malaysia: does poor adherence matter? Int J Pharm Sci. 2010; 2(1): 24–32.
- Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012; 6: 613–622. https://doi.org/10.2147/ppa.s34704
- Berg JS, Dischler J, Wagner DJ, Raia JJ, Palmer-Shevlin N. Medication compliance: a healthcare problem. Ann Pharmacother. 1993; 27(Suppl): S1–S24.
- DiMatteo MR. The role of effective communication with children and their families in fostering adherence to pediatric regimens. Patient Educ Couns. 2004; 55(3): 339–344. https://doi.org/10.1016/j.pec.2003.04.003
- Mulia N, Ye Y, Greenfield TK, Martinez P, Patterson D, Kerr WC, et al. Inequitable access to general and behavioral healthcare in the US during the COVID-19 pandemic: a role for telehealth? Prev Med. 2023; 169: 107426. https://doi.org/10.1016/j.ypmed.2023.107426
- Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. 2020; 20(1): 1193. https://doi.org/10.1186/s12889-020-09301-4
- Wei J, Hollin I, Kachnowski S. A review of the use of mobile phone text messaging in clinical and healthy behaviour interventions. J Telemed Telecare. 2011; 17(1): 41–48. https://doi.org/10.1258/jtt.2010.100322
- Khonsari S, Subramanian P, Chinna K, Latif LA, Ling LW, Gholami O. Effect of a reminder system using an automated short message service on medication adherence following acute coronary syndrome. Eur J Cardiovasc Nurs. 2015; 14(2): 170–179. https://doi.org/10.1177/1474515114521910
- Ollivier L, Romand O, Marimoutou C, Michel R, Pognant C, Todesco A, et al. Use of short message service to improve malaria chemoprophylaxis compliance after returning from a malaria endemic area. Malar J. 2009; 8: 236. https://doi.org/10.1186/1475-2875-8-236
- Vervloet M, van Dijk L, Santen-Reestman J, van Vlijmen B, Bouvy ML, de Bakker DH. Improving medication adherence in type 2 diabetes patients through real-time medication monitoring combined with short message service reminders: a randomized controlled trial. BMC Health Serv Res. 2011; 11: 5. https://doi.org/10.1186/1472-6963-11-5
- Li X, Hu J, Yao Y, Zuo C, Wang Z, Li X, et al. Evaluation of pharmacist-led telemedicine medication management for hypertension during the COVID-19 pandemic: a pilot study. Front Public Health. 2022; 10: 1091484. https://doi.org/10.3389/fpubh.2022.1091484
- Jin J, Sklar GE, Oh VMS, Li SC. Factors affecting therapeutic compliance: a review from the patient’s perspective. Ther Clin Risk Manag. 2008; 4(1): 269–286. https://doi.org/10.2147/tcrm.s1458
- Gadkari AS, McHorney CA. Unintentional non-adherence to chronic prescription medications: how unintentional is it really? BMC Health Serv Res. 2012; 12: 98. https://doi.org/10.1186/1472-6963-12-98
- Ting CY, Zaidi Adruce S, Loo SC, Ting H, Tnay J. Interventions on improving medication adherence in Malaysia: a mini review. J Young Pharm. 2019; 11(2): 122–125. https://doi.org/10.5530/jyp.2019.11.27
- Haynes RB, Taylor DW, Sackett DL, Gibson ES, Bernholz CD, Mukherjee J. Can simple clinical measurements detect patient noncompliance? Hypertension. 1980; 2: 757–764. https://doi.org/10.1161/01.hyp.2.6.757
- Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthma treatment: a three-month follow-up study. Respir Med. 2010; 104(2): 166–171. https://doi.org/10.1016/j.rmed.2009.10.003
- Sealed Envelope Ltd. Create a blocked randomization list [Internet]. London: Sealed Envelope Ltd; 2017. Available from: https://www.sealedenvelope.com
- Ruby G, Cathy DD, Patrick RM, Daniel SS. Pill count, self-report, and pharmacy claims data to measure medication adherence in the elderly. Ann Pharmacother. 1998; 32: 749–754. https://doi.org/10.1345/aph.17423
- Agh T. Comparative analysis of medication possession ratio measures for adherence to single medication. Value Health. 2016; 19(7). https://doi.org/10.1016/J.JVAL.2016.09.777
- Pop-Eleches C, Thirumurthy H, Habyarimana JP, Zivin JG, Goldstein MP, de Walque D, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011; 25(6): 825-34. https://doi.org/10.1097/qad.0b013e32834380c1
- Franklin VL, Waller A, Pagliari C, Greene SA. A randomized controlled trial of Sweet Talk, a text-messaging system to support young people with diabetes. Diabet Med. 2006; 23(12): 1332–1338. https://doi.org/10.1111/j.1464-5491.2006.01989.x
- Schedlbauer A, Davies P, Fahey T. Interventions to improve adherence to lipid-lowering medication. Cochrane Database Syst Rev. 2010; (3): CD004371. https://doi.org/10.1002/14651858.cd004371.pub3
- van Dalem J, Krass I, Aslani P. Interventions promoting adherence to cardiovascular medicines. Int J Clin Pharm. 2012; 34(2): 295–311. https://doi.org/10.1007/s11096-012-9607-5
- Cutrona SL, Choudhry NK, Fischer MA, Servi A, Liberman JN, Brennan TA, et al. Modes of delivery for interventions to improve cardiovascular medication adherence. Am J Manag Care. 2010; 16(12): 929–942. https://pmc.ncbi.nlm.nih.gov/articles/PMC3115758/
- Bokolo Anthony J Jr. Use of telemedicine and virtual care for remote treatment in response to the COVID-19 pandemic. J Med Syst. 2020; 44(7): 132. https://doi.org/10.1007/s10916-020-01596-5
Please cite this article as:
Sze Wei Teh, Leong Seng Tan, Khai Shing Chew, Ai Luan Teoh and Kheng Kai Chan, The Impact of Telehealth on Medication Adherence Among Patients with Hypertension at Hospital Bukit Mertajam. Malaysian Journal of Pharmacy (MJP). 2025;2(11):48-55. https://mjpharm.org/the-impact-of-telehealth-on-medication-adherence-among-patients-with-hypertension-at-hospital-bukit-mertajam/