ABSTRACT
Background: Fungal infections pose significant health concerns globally, affecting millions. Topical fungal infections are common and stubborn, requiring targeted treatments. Infection severity varies from asymptomatic to life-threatening, impacting patient’s quality of life. Fluconazole is the most widely used drug to treat fungal infections. Emulgels, which combine the properties of both gels and emulsions, offer several advantages over traditional semisolid formulations, including enhanced spreadability, easy removal, and a greaseless texture. Methods: Oil-in-water emulsions (E1-E16) were developed using the microemulsion method, utilizing light liquid paraffin and olive oil as the oil phase, along with Tween 80 and Span 80 as emulsifying agents based on RHLB values. The emulsions were evaluated for drug content, visual characteristics, and globule size. Subsequently, sixteen emulgel formulations (F1-F16) were prepared by incorporating the emulsions into hydrophilic gels of HPMC K100M and Carbopol 940 separately. The emulgels were subjected to evaluation for drug content, pH, viscosity, spreadability, extrudability, in vitro diffusion, ex vivo drug release, skin irritation, and antifungal studies. Results: The drug content of emulgels ranged from 94.6% to 98.5%, pH values from 5.65 to 6.16, and viscosity from 1106 to 1866 cps. Notably, the optimized formulation F3 exhibited ideal physicochemical properties and achieved a drug release of 95.50% in 12 hours, demonstrating a controlled release mechanism. The ex vivo drug release was 89.5% across lbino Wistar Rat abdominal skin in 12 hours. Skin irritation tests revealed the absence of any irritation, and antifungal study proved the efficacy of the developed emulgel F3 against fungi. Conclusion: Although further safety and toxicity assessments are warranted to establish the formulation’s suitability for human use, this study underscores the potential of emulgel systems in enhancing the topical delivery of hydrophobic drugs like fluconazole for effective therapy.
INTRODUCTION
Transdermal delivery systems are designed to deliver an active ingredient (drug substance) across the skin and into systemic circulation, while topical delivery systems are designed to deliver the active ingredient to local tissue. To obtain topical or systemic effects, topical preparations are applied to the surface of the skin. Topically applied dermal and transdermal delivery systems may replace needles required to administer several medications, offering benefits such as avoiding first-pass hepatic metabolism, gastric degradation, and frequent dosing. Conventional topical systems, such as ointments and creams, are less effective for skin permeation due to their poor efficiency and are associated with side effects such as burning, contact dermatitis, and stinging sensations owing to uncontrolled release of the drug [1]. Emulgel is a mixture of gels and emulsions. It consists of emulsions, either oil-in-water (o/w) or water-in-oil (w/o), which are gelled by combining them with a gelling agent. Emulgels are more effective in therapeutic aspects than regular gels. The conversion of an emulsion into a gel is responsible for the improved stability and penetrability of the emulsion. Moreover, this system exhibits dual controlled release, which is attributed to both the emulsion and the gel. Emulgel also prolongs the contact period of medication on the skin due to its mucoadhesive properties. Other advantages of emulgel include easy incorporation of drugs, augmented drug loading capacity, production feasibility (with simple and short processing steps), low preparation cost, avoidance of first-pass metabolism and gastrointestinal incompatibility, improved patient compliance, suitability for self-medication, and selectivity for a specific site [2]. Fluconazole is an antifungal drug that fights opportunistic infections in people with HIV and severe fungal infections. it belongs to the triazole class of antifungal agents and overcomes the side effects associated with other antifungal drugs like ketoconazole, amphotericin B, clotrimazole, and miconazole. Only 10% of fluconazole is protein bound, and it exhibits excellent tissue penetration, with a half-life of 27 to 34 hours. However, fluconazole has some side effects in oral and parenteral dosage forms, such as headache, diarrhea, nausea, dizziness, and stomach pain, as well as disadvantages like first-pass metabolism through the liver and excretion though the kidneys [3]. Theoretically, there is no need for systemic administration of a drug that is used to treat a localized condition. Therefore, a major challenge faced by healthcare providers is finding a suitable route of administration and a vehicle that can effectively deliver localized drugs while causing fewer systemic side effects. This need has emphasized the importance of developing a topical dosage form, specifically an emulgel, for fluconazole.
METHODS
Fluconazole was obtained as a gift sample from Dr Reddy’s Laboratories, Hyderabad. Carbopol 934 and Carbopol 940 were procured from Hi Media Laboratories Pvt. Ltd., Mumbai. HPMC K4M and HPMC K100M were purchased from Shin Etsu Chemical Pvt. Ltd., New Delhi. Light liquid paraffin was obtained from Rankem Laboratories Pvt. Ltd., Maharashtra. Olive oil was sourced from Figaro Deoleo Global, Spain. All additional chemicals and reagents used were of analytical grade, commercially available, and used without any further processing.
Preformulation Studies
A) Partition coefficient study (kow)
The partition coefficient of fluconazole was determined using the “shake flask method” with a water- n-octanol system. 20 mL of n-octanol and 20 mL of phosphate buffer solution (pH 7.4) were taken in separate beakers, and 200 mg of fluconazole was weighed.
In 20 mL n-octanol, the drug (200 mg) was dissolved slowly by continuous stirring with constant speed until saturation was achieved. In a 100 mL separation funnel, both n-octanol saturated with the drug and the phosphate buffer solution (pH 7.4) were transferred and shaken vigorously for 30 mins, then kept aside for 2 hrs. The two solutions were then separated and measured at 261 nm using a UV spectrophotometer. The concentration of the drug in the respective solutions was calculated using the following formula [4]:

Preparation of Fluconazole Emulsion Using the Microemulsion Method
A) Preparation of aqueous phase
20 mL of aqueous phase (water) was taken. The amount of surfactant was calculated using the required HLB (RHLB), and the calculated quantity of Tween 80 (0.75 ml) was transferred to the beaker. Additionally, 0.2 mg of methylparaben was used as a preservative and was dissolved in 2.5 mL of propylene glycol. 250 mg of fluconazole was dissolved in 2 ml ethanol. Both mixtures were added to the beaker to form aqueous phase.
B) Preparation of oil phase
Light liquid paraffin (E1- E8) and olive oil (E9 – E16) were used as the oil medium to prepare the emulsion. For formulations E1 – E8, 3.75 mL of light liquid paraffin was taken, and the calculated amount of surfactant Span 80 (0.75 ml) was added and mixed to form oil phase. for formulations E9 – E16, 4 mL of olive oil was taken in a beaker, and the calculated amount of surfactant Span 80 (0.25 mL) was added and mixed to form the oil phase. The quantities of surfactant were calculated based on the required hydrophilic-lipophilic balance.
C) Emulsification
The aqueous phase and oil phase were separately heated to 70 oC, and then the oil phase was slowly added to the aqueous phase using a homogeniser with continuous stirring at 1000 rpm until an emulsion was obtained. The emulsion obtained was of oil in water type. The formulation of all emulsions (E1-E16) prepared is given in Table I.
C) Formulation of gel
25 mL of water was taken, and the calculated quantities of Carbopol 930 and Carbopol 940 were added and stirred at 600 rpm until a firm gel was obtained. Another 25 mL of water was taken, and the calculated quantities of HPMC K4M and HPMC K100M were added and stirred on a magnetic stirrer at 600 rpm, then stored overnight to achieve a firm gel.
Preparation of fluconazole topical emulgel
The prepared emulsions were mixed dropwise with the respective gel base separately, with continuous stirring on a magnetic stirrer at 600 rpm to obtain the emulgel. The pH was adjusted using 0.1 mL of triethanolamine. The prepared emulgels were packed in wide-mouth glass jars. The formulation of all emulgels (F1-F16) prepared is given in Table II [5].
Evaluation of fluconazole emulsion
A) Visual examination
The prepared emulsions were observed for microscopic images, colour, homogeneity, consistency, and phase separation [6].
B) Globule size determination
Calibration of ocular/eyepiece micrometer
The eyepiece micrometer was calibrated using a stage micrometer with a linear scale of 1mm divided into 100 equal parts engraved on it. Hence, one division of the stage micrometer is equal to 10 µm or 0.01mm. The eyepiece micrometer was calibrated by superimposing it on the stage micrometer and measuring the design overlapped. The formula used to calculate the calibration factor is:

For measuring particle size, one drop of emulsion was placed on a glass slide, and amaranth red colour was added, and covered with a coverslip. 50 drops were counted across different microscopic fields and the diameters of the particles were noted [7].
A) Drug content
Microemulsion equivalent to 10 mg of drug was taken (1 mL) in 10 ml volumetric flask containing 5 mL methanol and stirred for 30 minutes. The volume was made up to 10 mL with methanol. From the above solution, 0.1 mL was transferred to a 10 ml volumetric flask, and the volume was made up with methanol. The resultant solution was filtered through Whatman filter paper, and the absorbance of the solution was measured at 261 nm using a UV spectrophotometer. Drug content was calculated using the formula [8]:

Characterization of fluconazole topical emulgel
A) Visual examination
The prepared fluconazole topical emulgels were observed for colour, homogeneity, consistency, and phase separation [9].
B) pH
The pH of the fluconazole topical emulgel was measured using a digital pH meter in triplicate (Digisun Electronics, Hyderabad) [10].
C) Drug content
The drug content of the fluconazole emulgels was evaluated. 1 g of emulgel, expected to contain 5 mg of fluconazole, was placed in a beaker, and 80 mL of methanol was added. The mixture was warmed to 50 oC for 30 min. The emulgel methanolic solution was then filtered into a 100 ml volumetric flask, and the resulting drug solution was made up to volume using methanol. Afterwards, the sample was agitated in an ultrasonic bath for 5 min to facilitate complete drug dissolution. The absorbance of the prepared solution was measured at 261 nm using a UV–visible spectrophotometer. In addition, a pure drug sample (5 mg) was diluted by a factor of 100 using methanol, and its absorbance value was determined in triplicate [11]. The percentage drug content was calculated as follows:

According to the USP, drug content is satisfactory if 85 %–115 % of the drug is detected in the emulgel formulations.
D) Viscosity studies
The viscosity of all the prepared formulations was determined by using a Brook Field Viscometer (DV- III ultra) (Shimadzu Corporation Ltd., Japan). A cone and plate method with spindle no. 06 was used. Initially, the instrument was calibrated and maintained at 37 oC. Then, auto-zero was performed. An emulgel equivalent to 0.5 g was taken and placed on the plate. The spindle was allowed to run, and the viscosity of emulgels F1-F16 was measured at 50 rpm. The viscosity was measured in centipoise in triplicate (cps) [12].
E) Spreadability test
The emulgel formulation (1 g) was sandwiched between two glass slides, and a 50 g weight was placed over the upper glass slide until no further spreading was evident. The difference in the spread circle diameter before and after the application of the weight was recorded, depicting the spreadability of the emulgels F1-F16 in triplicate [13].

| Ingredients | Fluconazole emulsions | |||||||||||||||
| E1 | E2 | E3 | E4 | E5 | E6 | E7 | E8 | E9 | E10 | E11 | E12 | E13 | E14 | E15 | E16 | |
| Fluconazole (g) | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 | 0.25 |
| Liquid paraffin (mL) | 3.75 | 3.75 | 3.75 | 3.75 | 3.75 | 3.75 | 3.75 | 3.75 | – | – | – | – | – | – | – | – |
| Olive oil (mL) | – | – | – | – | – | – | – | – | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| Tween 80 (mL) | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.45 | 0.45 | 0.45 | 0.45 | 0.45 | 0.45 | 0.45 | 0.45 |
| Span 80 (mL) | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 | 0.75 |
| Propylene glycol (mL) | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 | 2.5 |
| Methyl paraben (mg) | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 | 0.2 |
| Triethanolamine (mL) | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
| Purified water (mL) | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 10 |
| Ingredients | Fluconazole Emulgels | |||||||||||||||
| F1 | F2 | F3 | F4 | F5 | F6 | F7 | F8 | F9 | F10 | F11 | F12 | F13 | F14 | F15 | F16 | |
| Carbopol 934 (g) | 1 | 1.5 | – | – | – | – | – | – | 1 | 1.5 | – | – | – | – | – | – |
| Carbopol 940 (g) | – | – | 1 | 1.5 | – | – | – | – | – | – | 1 | 1.5 | – | – | – | – |
| *HPMC K4M (g) | – | – | – | – | 1 | 1.5 | – | – | – | – | – | – | 1 | 1.5 | – | – |
| *HPMC K100M (g) | – | – | – | – | – | – | 1 | 1.5 | – | – | – | – | – | – | 1 | 1.5 |
| Purified water (mL) | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 | 30 |
| Fluconazole Emulsion (mL) | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 | 25 |
| Sl. No. | Emulgel codes | pH | Drug Content (%) | Viscosity (Cps) | Spreadability (cm) | Extrudability test (%) |
| 1 | F1 | 5.8 ± 0.1 | 94.9 ± 0.13 | 1653 ± 0.1 | 4.8 ± 0.19 | 89.0 ± 0.19 |
| 2 | F2 | 6.1 ± 0.2 | 96.6 ± 0.25 | 1855 ± 0.2 | 4.5 ± 0.26 | 82.1 ± 0.08 |
| 3 | F3 | 5.8 ± 0.1 | 98.6 ± 0.69 | 1810 ± 0.1 | 4.1 ± 0.37 | 93.2 ± 0.11 |
| 4 | F4 | 5.9 ± 0.2 | 96.4 ± 0.72 | 1866 ± 0.1 | 4.0 ± 0.44 | 92.5 ± 0.21 |
| 5 | F5 | 5.8 ± 0.2 | 96.2 ± 0.93 | 1120 ± 0.2 | 4.0 ± 0.59 | 87.5 ± 0.18 |
| 6 | F6 | 6.1 ± 0.1 | 97.4 ± 0.85 | 1246 ± 0.1 | 3.9 ± 0.66 | 85.6 ± 0.27 |
| 7 | F7 | 6.2 ± 0.2 | 96.7 ± 0.69 | 1132 ± 0.2 | 3.9 ± 0.71 | 87.3 ± 0.34 |
| 8 | F8 | 6.1 ± 0.2 | 97.4 ± 0.12 | 1276 ± 0.3 | 3.8 ± 0.86 | 87.0 ± 0.48 |
| 9 | F9 | 6.0 ± 0.1 | 96.2 ± 0.35 | 1325 ± 0.1 | 4.7 ± 0.11 | 88.3 ± 0.12 |
| 10 | F10 | 5.9 ± 0.2 | 97.8 ± 0.42 | 1742 ± 0.2 | 4.4 ± 0.29 | 87.5 ± 0.67 |
| 11 | F11 | 5.8 ± 0.1 | 96.6 ± 0.59 | 1253 ± 0.1 | 4.6 ± 0.36 | 87.6 ± 0.15 |
| 12 | F12 | 5.7 ± 0.2 | 98.2 ± 0.77 | 1298 ± 0.1 | 4.2 ± 0.85 | 87.0 ± 0.54 |
| 13 | F13 | 5.9 ± 0.2 | 98.2 ± 0.50 | 1106 ± 0.2 | 4.0 ± 0.12 | 91.8 ± 0.34 |
| 14 | F14 | 5.7 ± 0.1 | 97.2 ± 0.23 | 1227 ± 0.1 | 3.9 ± 0.15 | 89.4 ± 0.12 |
| 15 | F15 | 5.8 ± 0.1 | 96.7 ± 0.23 | 1286 ± 0.1 | 3.9 ± 0.19 | 90.9 ± 0.12 |
| 16 | F16 | 5.9 ± 0.2 | 94.6 ± 0.26 | 1392 ± 0.2 | 3.6 ± 0.25 | 90.4 ± 0.18 |
F) Extrudability test
The emulgel formulations were filled into standard capped collapsible aluminium tubes with a capacity of 20 g and sealed by crimping the end. The weights of the tubes were recorded. The tubes were placed between two glass slides and clamped. A 50 g weight was placed over the upper slide, and then the cap was removed. The amount of gel extruded was collected and weighed. The percentage of the gel extruded was calculated in triplicate. (> 90% extrudability: Excellent, > 80% extrudability: Good, and > 70% extrudability: Fair) [14].

G) In-vitro diffusion study
A Franz diffusion cell was used for in vitro diffusion studies. The study was carried out using a cellulose membrane. The day before experiment, the cellulose membrane was placed in phosphate buffer solution (pH 7.4) to remove impurities, then dried and used for diffusion studies. 30 mL of phosphate buffer solution (pH 7.4) was taken in the receptor compartment, maintained at 37 oC ± 0.5, and continuously stirred with a magnetic stirrer at 60 rpm. 1 gm of the fluconazole topical emulgel, equivalent to 5 mg of drug, was placed uniformly on a circular cellulose membrane in the donor compartment. The donor compartment was slowly fixed to the receptor compartment until the membrane just touched the release medium in the receptor side. Aliquots volumes of samples (1mL) were withdrawn every 1 hr and analysed for drug content. The study was carried out for 12 hrs. During each sampling, an equal volume of fresh diffusion medium was replaced to maintain sink conditions. The samples were then analyzed for cumulative drug release using a UV-Visible double beam spectrophotometer at 261 nm, with phosphate buffer solution (pH 7.4) used as a blank, in triplicate [15].
H) Ex-vivo permeation studies
Franz diffusion cells with a diffusional surface area of 1.76 cm2 were used to study the permeability of fluconazole emulgel. Institutional ethics committee permission was obtained as per the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) guidelines (Approval No: NETPC/CPCSEA/ IAEC/01/23) for carrying out the study on animals, especially male albino Wistar rat. Albino Wistar rats weighing 140 to 160 g were used. The rats were sacrificed using an anaesthetic method with isoflurane. After shaving the hair with a hair removal cream without damaging skin, a 5 × 5 cm patch of skin was excised from the abdominal region of sacrificed rat. The skin membranes were first hydrated for 30 mins in the phosphate buffer solution (pH 7.4) at room temperature (32 ±1 oC) to remove extraneous debris and leachable enzymes. The excised skin was placed between the donor and receptor compartments of the cells, with the dermal side in direct contact with the receptor medium. The permeation characteristics were evaluated for the optimised topical emulgel F3 and the marketed fluconazole formulation (Flucos 0.5% -Oaknet Healthcare Pvt. Ltd., Mumbai). The same procedure was used as in the in vitro release studies, except that the excised rat abdominal skin was used as a membrane. The statistical analysis of the obtained data was performed using One-Way ANOVA [16].
Kinetic study
The release kinetics were studied using various models, including zero-order plot, first-order plot, Higuchi plot, and Korsmeyer-Peppas plot. The best-fit model was confirmed by the value of the correlation coefficient being close to 1.
A) Zero-order model
Drug diffusion from dosage forms that do not disaggregate and release the drug slowly can be represented by the equation:

Rearrangement of equation (1) yields:

Where Qt is the amount of drug dissolved at time t, Q0 is the initial amount of drug in the solution (most times, Q0 = 0), and K0 is the zero-order release constant expressed in units of concentration/time. To study the release kinetics, data obtained from in vitro drug release studies were plotted as cumulative amount of drug released versus time.
B) First order model
This model has also been used to describe the absorption and/or elimination of some drugs, although it is difficult to conceptualize this mechanism theoretically. The release of the drug which follows first-order rate constant expressed by the equation:
Where C0 is the initial concentration of the drug, k is the first-order rate constant, and t is the time. The data obtained are plotted as log cumulative percentage of drug remaining versus time, which would yield a straight line with a slope of .
C) Higuchi model
A graph was plotted between cumulative percentages of drug released versus square root of time:
Where K is the constant reflecting the design variables of the system and t is the time in hours. Hence, the drug release rate is proportional to the reciprocal of the square root of time [17].
D) Korsmeyer-Peppas model
A simple relationship which described drug release from a polymeric system has been derived by Korsmeyer and co-workers [42]. To find out the mechanism of drug release, first 60% drug release data were fitted in Korsmeyer-Peppas model.
Where

is a fraction of drug released at time t, k is the release rate constant, and n is the release exponent. A value of 0.45 ≤ n corresponds to a Fickian diffusion mechanism, 0.45 < n < 0.89 to non-Fickian transport, n = 0.89 to Case II (relaxation) transport, and n > 0.89 to super case II transport [18].
Skin irritation test
Institutional ethics committee permission was obtained as per the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) guidelines (Approval No: NETPC/CPCSEA/ IAEC/01/23) for carrying out the study on animals. The skin irritation study was carried out on six healthy albino Wistar rats (200-250 g) of either sex, and no injuries or skin disorders were observed. Two groups (n=3) of rats were used in the study. The animals were maintained on standard animal feed and had free access to water. One day prior to starting the study, hair was shaved from the backs of rats, and an area of 4 cm² was marked on both sides, one side served as the control while the other side was the test. On the control side, a standard irritant formalin solution (0.8 %) was smoothly applied with cotton swab. The prepared emulgel was applied to the test side and left for 7 days, during which the site was observed for any sensitivity or reactions, which were graded as 0, 1, 2, 3, or for no reaction, slightly patchy erythema, slight but confluent or moderate but patchy erythema, and severe erythema with or without edema, respectively, according to the Draize score test. A similar procedure was used to check the skin irritation of the marketed product in albino Wistar rats, and observations were recorded [19].
Anti-fungal studies (zone of inhibition against Candida albicans)
A) Preparation of Inoculum
Four to five colonies of standard Candida albicans strains were selected and suspended in normal saline (2 ml) and mixed vigorously. The turbidity of the fungal suspension was maintained homogeneously using the 0.6-meq McFarland standards. Streaks were then made on the Sabouraud dextrose agar plate by dipping a sterile swab into the prepared fungal suspension to create a lawn culture.
B) Disk Diffusion Method
Sterile filter paper discs of 5 mm in diameter were soaked with 100 µL of the optimised fluconazole topical emulgel F3 (test) and pure drug as positive control samples, respectively. The soaked paper disks were placed on the inoculated Sabouraud dextrose agar plates. The inoculated plates were incubated at 24 ±2 oC for 48 hrs and then examined for their respective zones of inhibition. The radius of the zone of inhibition was calculated. [20]
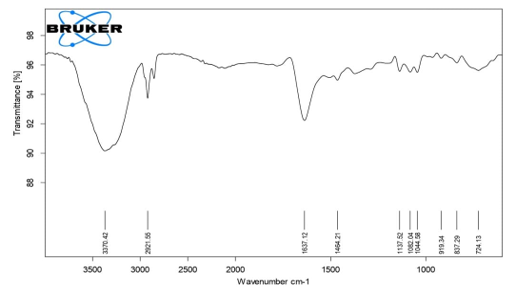
C) Fourier Transform Infrared spectroscopy (FTIR)
FTIR studies were performed to assess the possibility of interactions between the drug, polymer, and excipients. FTIR studies were performed on pure fluconazole and the optimized emulgel formulation F3 (Carbopol 940 + liquid paraffin). The fluconazole emulgels were mixed with potassium bromide (KBr) pellets. The FTIR spectrum was recorded in the wavelength range of 4000 to 400 cm-1 [21].
RESULT AND DISCUSSION
Preformulation studies
A) Partition coefficient
The partition coefficient of fluconazole (20 mg/mL) between n-octanol and phosphate buffer (pH 7.4) was found to be Kow = 1.16 ± 0.2, which is close to the reported value of 1.76 [22]. Ashok et al. reported a similar value (1.01 ± 0.01) for fluconazole between octanol and water, which is useful for understanding its in vivo behavior [23]. The obtained value indicates that the drug is slightly more soluble in the lipid phase than in the aqueous phase, suggesting it traverses the stratum corneum mainly via the intercellular route. A Kow < 3 reflects a good balance between lipophilicity and hydrophilicity, favorable for effective absorption across biological membranes.
Preparation of fluconazole topical emulgel
Fluconazole-loaded emulsion was prepared using the microemulsion method. Light liquid paraffin and olive oil were used as oily medium to prepare o/w emulsion. Emulsifiers like Tween 80 and Span 80 were used, and their amounts were calculated based on RHLB for stable emulsion formulation. A total of 16 emulsions formulations,a E1 – E8 (using light liquid paraffin as the oil medium) and E9 – E16 (olive oil as the oil medium), were prepared. Fluconazole emulsions were prepared using a homogenizer.
Four different polymers, Carbopol 934, Carbopol 940, HPMC K4M, and HPMC K100M, with two different ratios (0.5g, 1.0g), were used to form gels. A total of 16 emulgel formulations were obtained (F1- F16). The prepared emulsions were added to the gels by mixing on a magnetic stirrer to obtain emulgels. The details are stated in Table I and II.
Evaluation of fluconazole emulsion
A) Visual examination
The formulations E1-E8 exhibited a pale-yellow colour, while E9-E16 were milky white. The homogenesity and consistency of all formulations E1-E16 was excellent, and no phase separation was observed in any of the prepared formulations. All prepared formulations showed acceptable results.
B) Globule size analysis
Globule size analysis was conducted for all the prepared emulsion E1-E16 using optical microscopy. The dispersed globule size was found to be between 23-26.2 µm, indicating that the adopted method was suitable. The globule size of emulsions prepared using liquid paraffin as the medium was slightly smaller than that of globules obtained with olive oil as the medium.
Evaluation of fluconazole emulgels
A) Visual Examination
All prepared emulgels (F1–F16) were visually evaluated for colour, homogeneity, consistency, and phase separation. Formulations with lower polymer concentrations appeared creamy white, while those with higher polymer concentrations were thicker and creamy white. All emulgels exhibited excellent homogeneity and consistency, with no signs of phase separation, indicating good physical stability. These observations are in agreement with the findings of Dalia Abd El-Rhman et al., who reported fluconazole emulgels as yellowish to white, viscous, creamy preparations with a smooth, homogeneous texture and glossy appearance [24].
B) pH
The pH of fluconazole topical emulgels was measured using a pH meter and found to range from 5.7 ± 0.2 to 6.2 ± 0.1. These values fall within the normal skin pH range (5.5–6.5), indicating that the formulations are likely to be non-irritating. The results are presented in Table III. According to previous studies, maintaining a slightly acidic pH (4.5–6.5) is crucial for compatibility with the skin’s natural acid mantle, which supports barrier function, prevents irritation, and enhances both the stability and efficacy of the active ingredients in emulgels [25].
C) Drug content
It was observed that the drug content in the prepared emulgels was satisfactory, with the drug uniformly distributed throughout all the emulgels. The percentage of drug content was found to be between 94.6 ± 0.26 to 98.6 ± 0.69. The results are shown in Table III.
D) Viscosity
Formulations F1, F2, F9, and F10 prepared using Carbopol 934 exhibited viscosities ranging from 1325 ± 0.1 to 1855 ± 0.2 cps, whereas F3, F4, F11, and F12 formulated with Carbopol 940 showed viscosities between 1253 ± 0.1 and 1866 ± 0.1 cps. Emulgels containing HPMC K4M (F5, F6, F13, and F14) demonstrated viscosities of 1106 ± 0.2 to 1246 ± 0.1 cps, while those containing HPMC K100M (F7, F8, F15, and F16) exhibited viscosities in the range of 1132 ± 0.2 to 1392 ± 0.2 cps. The highest viscosity was observed for formulation F3 (1866 ± 0.2 cps), and the lowest for formulation F13 (1106 ± 0.2 cps). Overall, Carbopol 940 produced emulgels with the highest viscosity, whereas HPMC K4M resulted in the lowest. These findings are consistent with previous reports by Rabia B et al. and Khangar PK et al. [26, 27]. The higher viscosity observed in HPMC K100M formulations compared to HPMC K4M can be attributed to its greater molecular weight, which enhances chain entanglement and gel strength [28]. Similarly, Carbopol (polyacrylic acid) polymers are well known for forming highly viscous gels; among them, Carbopol 940 typically produces higher viscosities than Carbopol 934 due to its increased degree of cross-linking [29]. The results are shown in Table III.
E) Spreadability
The spreadability of the prepared emulgels ranged from 3.6 ± 0.25 cm (F16) to 4.8 ± 0.19 cm (F1), indicating that all formulations were easily spreadable under minimal shear stress. These values reflect favorable rheological characteristics for topical application, ensuring uniform drug distribution and ease of use (Table III). Spreadability is a critical parameter influencing the ease of application, dose uniformity, and patient compliance [30, 31]. Formulations with higher spreadability require less force during application, thereby enhancing patient comfort [32].
In the present study, emulgels containing HPMC K4M exhibited slightly higher spreadability, whereas those formulated with HPMC K100M or Carbopol 940 showed lower values, which can be attributed to their higher viscosity and stronger gel network formation. These observations are consistent with reports by Revati BC et al. and Alex NM et al., who demonstrated that increasing polymer viscosity leads to reduced spreadability due to enhanced internal resistance within the gel matrix [31, 33].
F) Extrudability test
Extrudability is a key parameter determining the ease of application and patient acceptability of topical emulgels. Formulations with excessively high consistency may resist extrusion, while those with very low viscosity may flow too readily; hence, achieving an optimal consistency is crucial for uniform and controlled extrusion. In the present study, the extrudability of all emulgel formulations (F1–F16) ranged from 82% to 93%, indicating satisfactory extrusion characteristics. These results suggest that all formulations can be conveniently dispensed from collapsible tubes without excessive force, ensuring user convenience and emphasizing that formulations with moderate viscosity facilitate both smooth extrusion and uniform application. The corresponding data are summarized in Table III.
G) In vitro diffusion studies
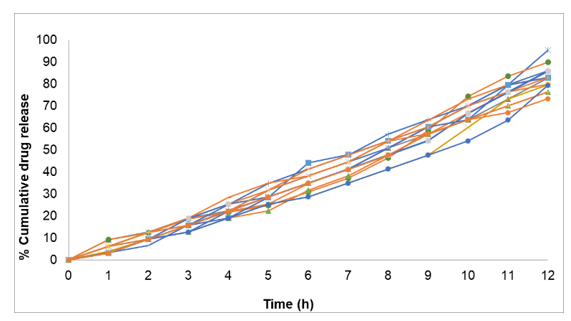
In-vitro diffusion studies demonstrated that all fluconazole emulgel formulations (F1–F16) exhibited cumulative drug release ranging from 76.66% to 95.5% at the end of 12 hrs (Figure I). The release profiles were found to be strongly influenced by the type of polymer used.
Formulations containing Carbopol 934 as the gelling agent released 82.90% (F1), 79.80% (F2), 83.10% (F9), and 76.60% (F10) of the drug after 12 hrs, whereas formulations with Carbopol 940 exhibited higher release values of 95.50% (F3), 89.90% (F4), 85.90% (F11), and 83.0% (F12). Although Carbopol 940 generally forms gels of higher viscosity than Carbopol 934, its greater cross-linking density and enhanced swelling capacity generate a more hydrated and porous matrix, facilitating faster drug diffusion. These findings are consistent with those of Kumud U et al., who reported higher drug release from Carbopol 940-based emulgels despite increased viscosity, due to improved matrix hydration and drug diffusivity [30]. This suggests that polymer structure and swelling behavior, rather than viscosity alone, predominantly govern drug release performance in emulgel systems.
Formulations prepared with HPMC K4M released 86.20% (F5), 83.10% (F6), 83.10% (F13), and 85.90% (F14) of the drug after 12 hrs, while those containing HPMC K100M exhibited comparatively lower release values of 86.10% (F7), 79.90% (F8), 79.50% (F15), and 73.40% (F16). The reduced release from HPMC K100M formulations may be attributed to its higher molecular weight and viscosity, leading to the formation of a denser gel matrix and a thicker diffusion barrier that retards drug transport. Conversely, the lower viscosity of HPMC K4M facilitates greater water penetration and faster diffusion through the gel network. Similar observations were reported by Revati BC et al. and Alex NM et al., who found that increasing polymer viscosity or employing higher molecular-weight grades (e.g., HPMC K100M) diminished drug release due to reduced matrix hydration and diffusivity [31, 33].
Overall, the release profile followed the order: Carbopol 940 > Carbopol 934 > HPMC K4M > HPMC K100M. Comparable trends were observed by Mona Piplani et al., who reported higher drug release (~89.56%) from a diclofenac potassium emulgel formulated with Carbopol 940 compared to an HPMC-based formulation (~84.45%) [34]. Based on its superior drug release and higher yield, the fluconazole emulgel F3 (Carbopol 940-based) was identified as the optimized formulation for further evaluation.
optimized emulgel F3 and fluconazole marketed product –
Flucos Gel 0.5%
| Formulation code | Zero order | First order | Higuchi | Korsmeyer-Peppas |
| r2** | r2** | r2** | n* | |
| F1 | 0.988 | 0.894 | 0.881 | 1.265 |
| F2 | 0.981 | 0.867 | 0.830 | 1.418 |
| F3 | 0.965 | 0.727 | 0.857 | 1.388 |
| F4 | 0.952 | 0.809 | 0.813 | 1.291 |
| F5 | 0.996 | 0.921 | 0.830 | 1.441 |
| F6 | 0.994 | 0.928 | 0.902 | 1.372 |
| F7 | 0.988 | 0.888 | 0.863 | 1.525 |
| F8 | 0.987 | 0.911 | 0.868 | 1.372 |
| F9 | 0.986 | 0.916 | 0.881 | 1.526 |
| F10 | 0.986 | 0.929 | 0.859 | 1.482 |
| F11 | 0.985 | 0.865 | 0.861 | 1.519 |
| F12 | 0.998 | 0.936 | 0.908 | 1.367 |
| F13 | 0.955 | 0.862 | 0.870 | 1.486 |
| F14 | 0.996 | 0.962 | 0.911 | 1.343 |
| F15 | 0.673 | 0.850 | 0.845 | 1.435 |
| F16 | 0.996 | 0.963 | 0.907 | 1.468 |
** r2 is correlation – coefficient
* n is the release exponent
| Formulation code | Score | |
| Day-1 | Day-7 | |
| Control | 0 | 0.5 |
| F3 | 0 | 0 |
| Marketed product | 0 | 0 |
0 = No reaction, 0.5 = slight patchy erythema
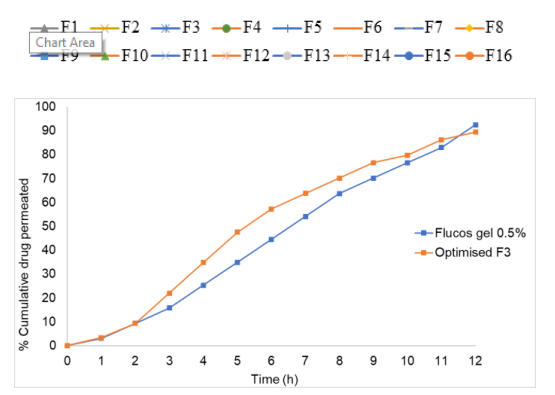
H) Ex-vivo permeation studies
The ex-vivo permeation profile of the optimized fluconazole emulgel (F3) was compared with that of the marketed formulation, Flucos Gel 0.5% (Oaknet Healthcare Ltd.), using excised albino Wistar rat abdominal skin (5 × 5 cm) as the permeation membrane. The study was conducted for 12 hrs, and the cumulative drug permeation was found to be 89.5% for the optimized formulation (F3) and 92.2% for the marketed product. The slightly lower permeation observed with the optimized formulation compared to the marketed product may be attributed to the structural barrier properties of the stratum corneum, where ceramides and other lipids form a bilayer arrangement that restricts diffusion. [35] The reduced ex vivo permeation relative to in-vitro release (using a cellophane membrane) further supports the role of the skin barrier in modulating drug transport.
Statistical evaluation using one-way ANOVA yielded a p-value of 0.000252, indicating a statistically significant difference (p < 0.05) in permeation, thereby confirming that the optimized emulgel facilitated effective drug transport across rat skin. The ex-vivo permeation profiles of both formulations are illustrated in Figure II.
I) Flux
For emulgels F1, F2, F9 and F10 (prepared using Carbopol 934 polymer), flux values were 2.51, 2.38, 2.29 and 2.26 µg/cm²/hr respectively; flux decreased with increasing polymer concentration and gel thickness. A similar trend was observed for the other emulgels. Emulgels F3, F4, F11 and F12 (using Carbopol 940) had flux values of 2.61, 2.55, 2.47 and 2.36 µg/cm²/hr, respectively. Those with HPMC K4M (F5, F6, F13, F14) showed fluxes of 2.54, 2.47, 2.36 and 2.25 µg/cm²/hr; and those with HPMC K100M (F7, F8, F15, F16) exhibited flux values of 2.54, 2.38, 2.21, and 2.12 µg/cm²/hr. The optimized formulation F3 demonstrated the highest flux of 2.61 µg/cm²/hr. In the ex vivo permeation study, flux for F3 was 2.40 µg/cm²/hr, whereas the marketed product had 2.59 µg/cm²/hr, indicating that the developed emulgel possessed nearly equivalent permeation efficiency to the commercial formulation. This relationship between polymer concentration, viscosity, and drug flux has been demonstrated in hydrogel systems, where increased polymer content and cross‑linking density reduce drug release rates by restricting diffusion pathways [36].
J) Kinetic studies
The kinetic analysis of the fluconazole topical emulgel formulations is summarized in Table IV. The results indicated that the selected formulations predominantly followed zero-order kinetics, as evidenced by higher correlation coefficient values (r² = 0.9529–0.9986) compared to first-order kinetics (r² = 0.7272–0.9635). When the release data were plotted according to Higuchi kinetics, fairly linear profiles were obtained, with correlation coefficients ranging from 0.8131 to 0.9110, suggesting that drug release was proportional to the square root of time and therefore diffusion-controlled. Further analysis using the Korsmeyer–Peppas model yielded release exponent (n) values ranging from 0.6797 to 0.7950, indicating non-Fickian (anomalous) release behavior, where drug release is governed by a combination of diffusion and polymer chain relaxation. These findings are consistent with previously reported fluconazole emulgel systems, where Banyal et al. observed n = 0.5483–0.6508 and another study reported n = 0.5852–0.6509 [37, 38]. The slightly higher n values in the
present study may reflect differences in gel/emulgel matrix composition and polymer network dynamics. Overall, these observations indicate that drug release from the fluconazole topical emulgels is diffusion-controlled and follows zero-order kinetics, ensuring a sustained and controlled release profile suitable for topical delivery.
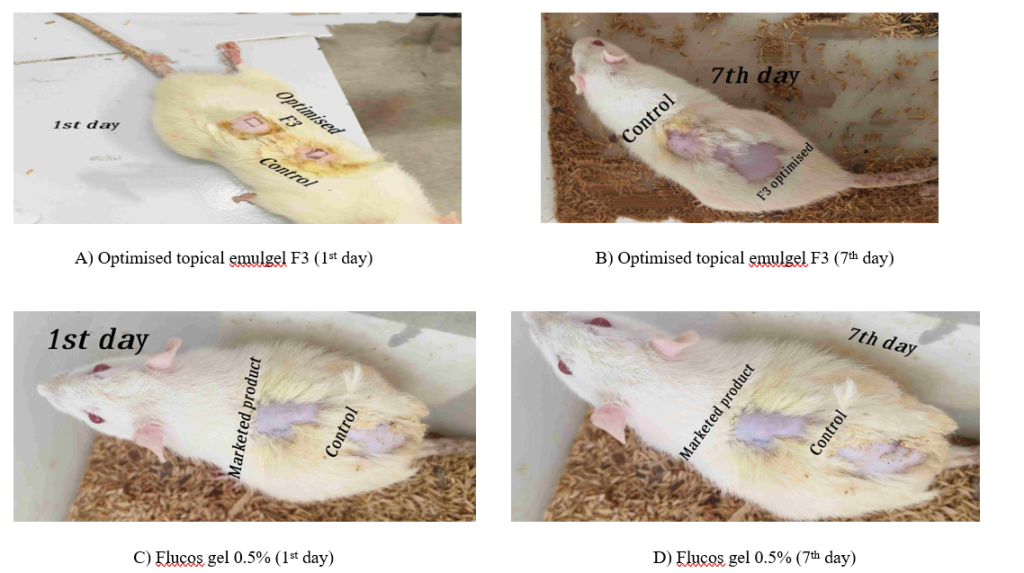
K) Skin irritation studies
Albino Wistar rats (200–250 g) of either sex were selected for the skin irritation study. The dorsal area (2 × 2 cm²) was shaved using a depilatory agent. The optimized fluconazole emulgel (F3) was applied to one side as the test formulation, while the standard reference was applied to the opposite side. The application sites were observed over seven days for signs of erythema and edema. The results demonstrated that the optimized emulgel F3 was well tolerated, with no observable allergic or irritant reactions, whereas the standard showed minimal response. The Draize score after 7 days was 0 for F3 and 0.5 for the standard, confirming that F3 was non-irritant (Table V, Figure III). These findings are consistent with previously reported studies on topical emulgels, such as the Naproxen-eugenol emulgel, which exhibited no irritation in rats over three days, and emulgels developed for atopic dermatitis, which showed no erythema or edema at any site. Collectively, these results confirm that the optimized emulgel F3 is safe and well-tolerated for topical application under the conditions tested. [39, 40]
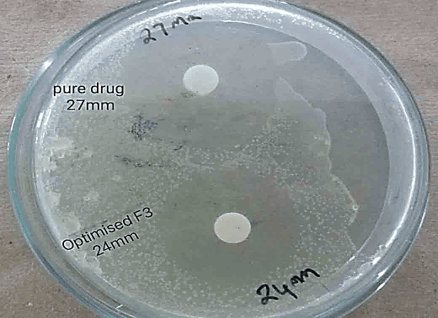
L) Antifungal studies
The antifungal efficacy of the optimised emulgel (F3) and pure drug was measured using the disk diffusion technique. The inhibitory zone diameters of the respective samples were measured at transitional points where the growth of C.albicans abruptly decreased. The areas were distinguished by a marked decrease in colony sizes. The diameters of the zones were measured after 48 hrs. For the optimised formulation F3, the diameter for the zone of inhibition was 24 mm, and whereas for the pure drug it was 27 mm, thereby proving the antifungal efficacy of the developed emulgel F3 (Figure IV). In comparison, earlier disk diffusion studies of fluconazole against C. albicans reported interpretive zone diameters of ≥20 mm (for a 25 µg disk) and ≥27 mm (for a 50 µg disk) to indicate susceptibility [41]. Thus, the 27 mm value for the pure drug aligns well with established susceptibility thresholds, while the 24 mm value for F3, although slightly lower, still falls well within a strong activity range—thereby supporting the developed emulgel’s promising antifungal potential.
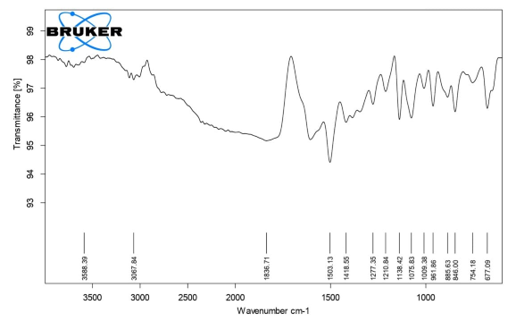
M) Fourier Transform Infrared spectroscopy (FTIR)
In the present study IR Spectra of the pure drug and formulations F3, were studied in detail. In the spectra, the drug showed characteristic absorption bands at almost the same positions with negligible variation compared to the IR of pure sample, thus clearly suggesting that the drug is in its normal form even in presence of excipients and has not undergone any kind of interactions. The spectra are shown in Figures V, VI.
CONCLUSION
This study investigates the design and characterization of fluconazole topical emulgels, highlighting various preformulation aspects and their alignment with existing literature. Employing the microemulsion method, oil/water emulsions of fluconazole were successfully developed using light liquid paraffin and olive oil. The subsequent preparation of fluconazole emulgels involved dispersing emulsions in various gelling agents, including Carbopol 940 and HPMC. Characterization results of drug content, pH, spreadability, viscosity, and extrudability of the emulgels were satisfactory. The optimal formulation F3 demonstrated a drug release of 95.50% over 12 hrs in in vitro diffusion studies. Skin irritation assessments confirmed the non-irritant nature of the optimized formulation. Antifungal efficacy was validated against C. albicans, exhibiting superior activity relative to the pure drug. Overall, fluconazole topical emulgel F3 presents a promising formulation, warranting further pharmacokinetic evaluation in appropriate test models.
ACKNOWLEDGEMENT
The authors are thankful to Mr. Mahendra, Dr. Redddy’s Laboratories, Hyderabad, Telangana for providing a gift sample of fluconazole to carry out the research work. We express our appreciation and honest thanks to Dr. R.H. Udupi for his help and encouragement during the course of this study.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCE
- Debjit B, Harish G, Pragati K, Duraivel S. Recent advances in novel drug delivery system. Pharma Innov. 2012;1(9):12-3. https://www.thepharmajournal.com/archives/2012/vol1issue9/PartA/1.1.pdf
- Hardenia A, Jayronia S, Jain S. Emulgel: An emergent tool in topical drug delivery. Int J Pharm Sci Res. 2014;5(5):1653-60. http://doi.org/10.13040/IJPSR.0975-8232.5(5).1653-60
- Kalia YN, Guy RH. Modeling transdermal drug release. Adv Drug Deliv Rev. 2001; 4(8):159-72. https://doi.org/10.1016/s0169-409x(01)00113-2
- European pharmacopoeia, vol.2, 5th edition 2005, Publisher- Council of Europe, 2327 28.
- Manyam N, Kumar K. Formulation and evaluation of emulgels loaded extended release of trimethoprim. J Pharma Med Hea sci. 2018;1(1):78-86.
- Mahaparale GV. Formulation and evaluation of iornoxicam emulgels. Int J Pharmaceut Chem Anal. 2017;4(3):83-87. https://doi.org/10.18231/2394-2797.2017.0019
- Barkat, Ali, Khan, Naveed B, Akhtar M, Haji K, Haji M. Basics of pharmaceutical emulsions: A review. Afr J Pharm Pharmacol. 2011;5(25):2715-25. https://doi.org/10.5897/AJPP11.698
- Hemanth G, Jyothi M, Richitha S, Sindhu S. Preparation and evaluation of fluconazole topical microemulsion. Am J Pharm Tech Res. 2018;8(4):327-41. https://doi.org/10.46624/ajptr.2018.v8.i4.026
- Bonacucina G, Cespi M, Palmieri GF. Characterization and stability of emulsion gels based on acrylamide/sodium acryloyl dimethyl taurate copolymer. AAPS Pharm Sci Tech. 2009;10:368-75. https://doi.org/10.1208/s12249-009-9218-1
- Nagai N, Iwamae A, Tanimoto S, Yoshioka C, Ito Y. Pharmacokinetics and anti inflammatory effect of a novel gel system containing ketoprofen solid nanoparticles. Biol Pharm Bull. 2015;38(12):1918-24. https://doi.org/10.1248/bpb.b15-00567
- Sudipta D, Haldar PK, Pramanik G. Formulation and evaluation of herbal gel containing clerodendrum infortunatum leaves extract. Int J Pharm tech Res. 2011;3(1):140-43. https://www.sphinxsai.com/Vol.3No.1/pharm_jan-mar11/pdf/JM11(PT=25)%20pp%20140-143.pdf
- Soumen P, SB Puranik. Formulation and evaluation of ketoprofen loaded nanoparticulate gel for topical delivery. IJPPR. 2018;11(3):250-60. https://ijppr.humanjournals.com/formulation-and-evaluation-of-ketoprofen-loaded-nanoparticulate-gel-for-topical-delivery/
- Mahendra, Rasik. Formulation and evaluation of topical anti-inflammatory herbal gel. Asian J Pharm Clin Res. 2019;12(7):252-55. https://doi.org/10.22159/ajpcr.2019.v12i7.33859
- Neelam I, Dinesh K. Design, development and evaluation of ethosomal gel of fluconazole for topical fungal infection. Int J Eng Sci Invention Res Dev. 2015 Feb;1(8):280-306. https://www.ijesird.com/wp-content/uploads/2024/05/february_paper_5.pdf
- Isik SO, Hatice YK, Gülten Kantarci SS, Tamer G, Gokhan E. Transdermal delivery of diclofenac sodium through rat skin from various formulations. AAPS Pharm Sci Tech. 2006;7(4):1-7. https://doi.org/10.1208/pt070488
- Kamal S, Sarabjeet S, Ajay ASN. Transdermal gels – An alternative vehicle for drug delivery. Int J Pharm Chem Biol Sci. 2013;3(3):495-03. https://www.ijpcbs.com/articles/transdermal-gelsan-alternativevehicle-for-drugdelivery.pdf
- AK Barupal, Vandana G, Suman R, Preparation and characterization of ethosomes for topical delivery of aceclofenac. Indian J Pharm Sci. 2010;72(5):582-86. https://doi.org/10.4103/0250-474x.78524
- Pisetpackdeekul P, Supmuang P, Pan-In P, Banlunara W, Limcharoen B, Kokpol C, et al. Proretinal nanoparticles: Stability, release, efficacy, and irritation. Int J Nanomedicine. 2016;11:3277-86. https://doi.org/10.2147/ijn.s111748
- Hala M, Alkhalidi, Khaled M, Hosny, Waleed Y, Rizg. Oral gel loaded by fluconazole-sesame oil nanotransfersomes: Development, optimization, and assessment of antifungal activity. Pharmaceutics. 2021;13(27):1-23. https://doi.org/10.3390/pharmaceutics13010027
- Shringirishi M, Mahor A, Gupta R, Prajapati S, Bansal K, Kesharwani P. Fabrication and characterization of nifedipine loaded β-cyclodextrin emulgels: An in-vitro and in vivo evaluation. J Drug Deliv Sci Technol. 2017;41:344-50. https://doi.org/10.1016/j.jddst.2017.08.005
- Nasir S, Muhammad I, Amjad H. Development and evaluation of scaffold based emulgels formulation for controlled drug delivery of naproxen and ibuprofen. Trop J Pharm Res. 2018;17(8):1465-74. https://doi.org/10.4314/tjpr.v17i8.2
- Pfizer Canada ULC. DIFLUCAN® (fluconazole) – Product Monograph. Kirkland (QC): Pfizer Canada ULC; [date of revision unknown]. Available from: https://www.pfizer.ca/sites/g/files/g10017036/f/201410/DIFLUCAN(2).pdf
- Ashok AH, Mahesh NM, Sushil S, Sachin K, Shweta P, Arun SD. Adsorption and partition studies of fluconzole. Asian J Research Chem. 2009;2(2):213-17. https://ajrconline.org/HTML_Papers/Asian%20Journal%20of%20Research%20in%20Chemistry__PID__2009-2-2-29.html
- Dalia Abd El-Rhman, Mohamed AE, Sally AA, Doaa AH. Pharmaceutical studies on fluconazole topical emulgel. ISRJ. 2014:4(5);1-13. https://www.researchgate.net/publication/271522749_PHARMACEUTICAL_STUDIES_ON_FLUCONAZOLE_TOPICAL_EMULGEL
- Lukić M, Pantelić I, Savić SD. Towards optimal pH of the skin and topical formulations: From the current state of the art to tailored products. Cosmetics. 2021;8(3):69:1-18. https://doi.org/10.3390/cosmetics8030069
- Rabia B, Yousra S, Nousheen A, Muhammad AM, Ambreen H, Anas MH. Influence of different gelling polymers on dexibuprofen gel formulation: In- vitro characterization and stability profile. Pak J Pharm Sci. 2023 Jan;36(1)(Special):287-93. https://doi.org/10.36721/PJPS.2023.36.1.SP.287-293.1
- Khangar PK, Magre S, Jain RK, Khare B, Jain V. Formulation and evaluation of flurbiprofen topical emulgels. Int J Med Sci Pharma Res. 2022;8(3):22-7. https://doi.org/10.22270/ijmspr.v8i3.55
- Echemi. HPMC in Pharmaceuticals: Understanding the key differences between HPMC K4M and K100M [Internet]. Echemi; [cited 2025 Nov 4]. Available from: https://www.echemi.com/cms/1299452.html#:~:text=Viscosity:%20The%20viscosity%20of%20HPMC,100%2C000%20cP%20at%202%25%20concentration
- Auda SH, El-Rasoul SA, Ahmed MM, Osman SK, El-Badry M. In-vitro release and in-vivo performance of tolmetin from different topical gel formulations. J Pharm Investig. 2015;45:311–17. https://doi.org/10.1007/s40005-015-0174-3
- Kumud U, Ritika A, Rukhsar K, Anup O, Himansu C. Formulation and characterization of terbinafine emulgel for superficial fungal infections. Research J Pharm and Tech. 2018;11(11): 5029-36. https://doi.org/10.5958/0974-360x.2018.00917.4
- Revati BC, Dhananjay MP, Vinod AB. Emulgel: A comprehensive review for novel topical drug delivery system. World J Pharm Pharm Sci. 2021;10(4):434-44.
- Bakhrushina EO, Anurova MN, Zavalniy MS, Demina NB, Bardakov AI, Krasnyuk II. Dermatologic gels spreadability measuring methods comparative study. Int J App Pharm. 2022;14(1):164-68. https://doi.org/10.22159/ijap.2022v14i1.41267
- Alex NM, Peter MN, Shital MM, Nicholas MN, Paul MN, Geoffrey KK, Agnes WM. Meloxicam emulgels for topical management of rheumatism: Formulation development, in vitro and in vivo characterization. Saudi Pharm J. 2021;29(4):351-60. https://doi.org/10.1016/j.jsps.2021.03.005
- Piplani M, Sharma K, Yadav R, Bhateja P, Devi A. Comparative study of different polymer based emulgel. Int J of Pharm Sci. 2024;2(3):129-36. https://doi.org/10.5281/zenodo.10781299
- Wertz PW. Current understanding of skin biology pertinent to skin penetration: skin biochemistry. Skin Pharmacol Physiol. 2013;26(4 6):217 26. https://doi.org/10.1159/000351949
- Briggs F, Browne D, Asuri P. Role of polymer concentration and cross linking density on release rates of small molecule drugs. Int J Mol Sci. 2022;23(8):4118;1-9. https://doi.org/10.3390/ijms23084118
- Banyal M, Sharma R, Bhatia A. Formulation and evaluation of fluconazole emulgel for topical drug delivery. World J Pharm Res. 2020;9(8):2093-100.
- Singh S, Patel D, Gupta R. Development and characterization of fluconazole loaded emulgel for cutaneous candidiasis. Asian J Pharm Pharmacol. 2018;4(3):307-315.
- Khan BA, Ahmad S, Khan MK, Hosny KM, Bukhary DM, Iqbal H, Menaa F. Fabrication and characterizations of pharmaceutical emulgel co-loaded with naproxen-eugenol for improved analgesic and anti-inflammatory effects. Gels. 2022;8(10):608. https://doi.org/10.3390/gels8100608
- Gómez-Farto A, Jiménez-Escobar AL, Pérez-González N, Castán H, Clares B, Arias-Santiago S, Montero-Vílchez T. Development of an emulgel for the effective treatment of atopic dermatitis: biocompatibility and clinical investigation. Gels. 2024;10(6):370. https://doi.org/10.3390/gels10060370
- Kirkpatrick WR, Turner TM, Fothergill AW, McCarthy DI, Redding SW, Rinaldi MG, et al. Fluconazole disk diffusion susceptibility testing of Candida species. J Clin Microbiol. 1998Nov;36(11):3429-3432. https://doi.org/10.1128/jcm.36.11.3429-3432.1998
- Talevi, A., Ruiz, M.E. (2021). Korsmeyer-Peppas, Peppas-Sahlin, and Brazel-Peppas: Models of Drug Release. In: The ADME Encyclopedia. Springer, Cham. 2021. https://doi.org/10.1007/978-3-030-51519-5_35-1
Please cite this article as:
Mohammed Sarfaraz, Manojkumar Raichur and Doddayya Hiremath, Fluconazole Emulgel: A Comprehensive Design and Characterization Study. Malaysian Journal of Pharmacy (MJP). 2026;1(12):36-48. https://mjpharm.org/fluconazole-emulgel-a-comprehensive-design-and-characterization-study/